J Clin Neurol.
2014 Jan;10(1):37-41.
Primary Position Upbeat Nystagmus during an Acute Attack of Multiple Sclerosis
- Affiliations
-
- 1Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. kkkim@amc.seoul.kr
Abstract
- BACKGROUND AND PURPOSE
Ocular manifestation is one of the frequent signs of an acute attack in multiple sclerosis (MS), although primary position upbeat nystagmus (PPUN) is rare. The purpose of this study is to determine the incidence of PPUN in MS and to determine the lesions that are responsible for this sign.
METHODS
The medical records of 120 MS patients with acute brain lesions were reviewed over a consecutive period of 9 years; of these, 6 patients were found to have PPUN. Other ocular motor abnormalities were analyzed in combination with upbeat nystagmus, video-oculographic findings, and lesions detected on brain MRI.
RESULTS
Lesions in the pontine tegmentum involving the medial longitudinal fasciculus (MLF) and ventral tegmental tract (VTT) were the most common, being observed in three of the six patients with PPUN. One patient exhibited caudal medullary lesions bilaterally affecting the paramedian portion of the posterior tegmentum, and two patients exhibited multiple lesions involving the pons with the cerebral peduncle or medulla. In five patients, other ocular motor dysfunctions, such as gaze-evoked nystagmus (n=3) and internuclear ophthalmoplegia (n=1), were found in combination with upbeat nystagmus.
CONCLUSIONS
PPUN is an infrequent, ocular manifestation noted during an acute attack of MS, and was observed in 5% of the present cases. Brainstem lesions in these cases primarily involved the pontine tegmentum and the caudal medulla. These findings support the theory that upbeat nystagmus is attributable to damage to the upward vestibulo-ocular reflex pathway related to the vestibular nucleus, VTT, and interconnecting pathways.
Keyword
MeSH Terms
Figure
-
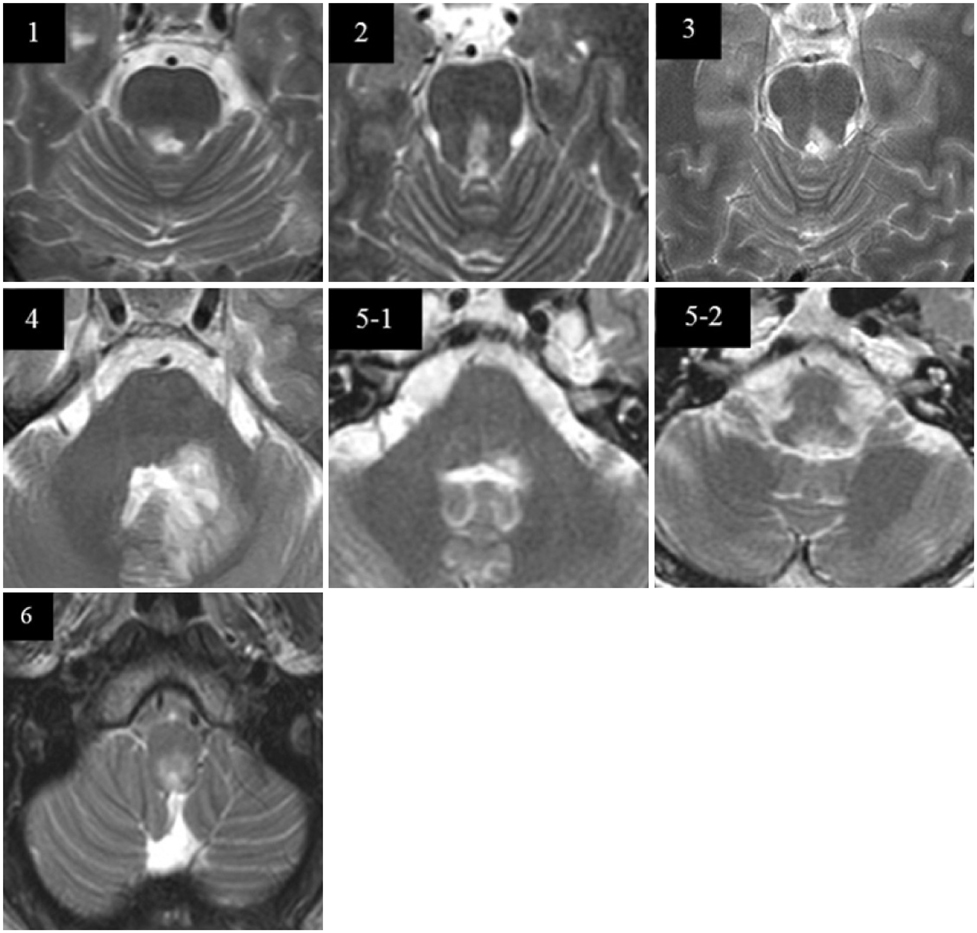
Fig. 1 Brain MRI scans of patients with upbeat nystagmus. Number on each figure represents patient's number.
Reference
-
1. Derwenskus J, Rucker JC, Serra A, Stahl JS, Downey DL, Adams NL, et al. Abnormal eye movements predict disability in MS: two-year follow-up. Ann N Y Acad Sci. 2005; 1039:521–523.
Article2. Fisher A, Gresty M, Chambers B, Rudge P. Primary position upbeating nystagmus. A variety of central positional nystagmus. Brain. 1983; 106:949–964.3. Hirose G, Kawada J, Tsukada K, Yoshioka A, Sharpe JA. Upbeat nystagmus: clinicopathological and pathophysiological considerations. J Neurol Sci. 1991; 105:159–167.
Article4. Gilman N, Baloh RW, Tomiyasu U. Primary position upbeat nystagmus. A clinicopathologic study. Neurology. 1977; 27:294–298.
Article5. Cox TA, Corbett JJ, Thompson HS, Lennarson L. Upbeat nystagmus changing to downbeat nystagmus with convergence. Neurology. 1981; 31:891–892.
Article6. Chen L, Gordon LK. Ocular manifestations of multiple sclerosis. Curr Opin Ophthalmol. 2005; 16:315–320.
Article7. Solingen LD, Baloh RW, Myers L, Ellison G. Subclinical eye movement disorders in patients with multiple sclerosis. Neurology. 1977; 27:614–619.
Article8. Ranalli PJ, Sharpe JA. Upbeat nystagmus and the ventral tegmental pathway of the upward vestibulo-ocular reflex. Neurology. 1988; 38:1329–1330.
Article9. Pierrot-Deseilligny C, Milea D. Vertical nystagmus: clinical facts and hypotheses. Brain. 2005; 128:1237–1246.
Article10. Kim JS, Yoon B, Choi KD, Oh SY, Park SH, Kim BK. Upbeat nystagmus: clinicoanatomical correlations in 15 patients. J Clin Neurol. 2006; 2:58–65.
Article11. Benjamin EE, Zimmerman CF, Troost BT. Lateropulsion and upbeat nystagmus are manifestations of central vestibular dysfunction. Arch Neurol. 1986; 43:962–964.
Article12. Kattah JC, Dagi TF. Compensatory head tilt in upbeating nystagmus. J Clin Neuroophthalmol. 1990; 10:27–31.13. Ohkoshi N, Komatsu Y, Mizusawa H, Kanazawa I. Primary position upbeat nystagmus increased on downward gaze: clinicopathologic study of a patient with multiple sclerosis. Neurology. 1998; 50:551–553.
Article14. Saito T, Aizawa H, Sawada J, Katayama T, Hasebe N. Lesion of the nucleus intercalatus in primary position upbeat nystagmus. Arch Neurol. 2010; 67:1403–1404.
Article15. Munro NA, Gaymard B, Rivaud S, Majdalani A, Pierrot-Deseilligny C. Upbeat nystagmus in a patient with a small medullary infarct. J Neurol Neurosurg Psychiatry. 1993; 56:1126–1128.
Article16. Adamec I, Gabelić T, Krbot M, Ozretić D, Milivojević I, Habek M. Primary position upbeat nystagmus. J Clin Neurosci. 2012; 19:161–162.
Article17. Kastrup O, Maschke M, Keidel M, Diener HC. Presumed pharmacologically induced change from upbeat- to downbeat nystagmus in a patient with Wernicke's encephalopathy. Clin Neurol Neurosurg. 2004; 107:70–72.
Article18. Janssen JC, Larner AJ, Morris H, Bronstein AM, Farmer SF. Upbeat nystagmus: clinicoanatomical correlation. J Neurol Neurosurg Psychiatry. 1998; 65:380–381.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Upbeat Nystagmus: Clinicoanatomical Correlations in 15 Patients
- Upbeat Nystagmus in Association with Wall-Eyed Bilateral Internuclear Ophthalmoplegia
- Transient Upbeat Nystagmus Due to Unilateral Pontine Infarction
- Mechanism of Downbeat Nystagmus While Normal Subjects HaveHead Upside-down Position in Darkness
- Primary Position Downbeat Nystagmus During Acute Vestibular Migraine
