J Rhinol.
2017 Nov;24(2):112-117. 10.18787/jr.2017.24.2.112.
Endoscopic Removal of Retained a Wooden Foreign Body Causing Persistent Intraorbital Inflammation
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Dankook University, College of Medicine, Cheonan, Korea. entdocjung@daum.net
- KMID: 2398829
- DOI: http://doi.org/10.18787/jr.2017.24.2.112
Abstract
- An intraorbital foreign body can cause a variety of signs and symptoms depending on size, location, and composition and can be classified as metal, inorganic, or organic depending on composition. An intraorbital organic foreign body, such as wood, can cause severe inflammation. An intraorbital foreign body is not only difficult to detect, but also can cause severe complications such as orbital cellulitis, orbital abscess, optic nerve injury, and extraocular muscle injury. A wooden foreign body can be very difficult to detect, even if computed tomography (CT) or magnetic resonance imaging (MRI) is used. Therefore, clinical suspicion based on history taking, physical examination, and radiological examination is essential for diagnosis of intraorbital wooden foreign body. We report a case of repeated intraorbital inflammation due to a retained wooden foreign body in a healthy 56-year-old male patient, who was treated with a combination of intravenous antibiotics and transnasal endoscopic foreign body removal.
Keyword
MeSH Terms
Figure
-
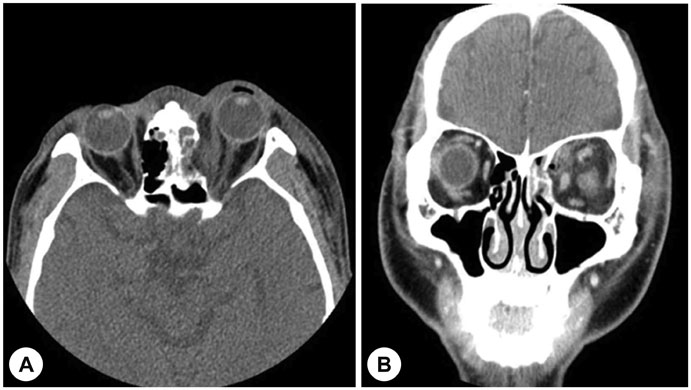
Fig. 1 Preoperative axial (A) and coronal (B) computerized tomography (CT) scans show diffuse air bubble with soft tissue swelling, haziness of left ethmoid sinus and medial blow out fracture.

Fig. 2 Axial (A) and coronal (B) computerized tomography (CT) scans performed 1 month after wooden penetrating injury show high density material that may outline the suspected retained wooden foreign body (arrow).

Fig. 3 Photograph of the removed wooden foreign body, sized 18×5 mm.
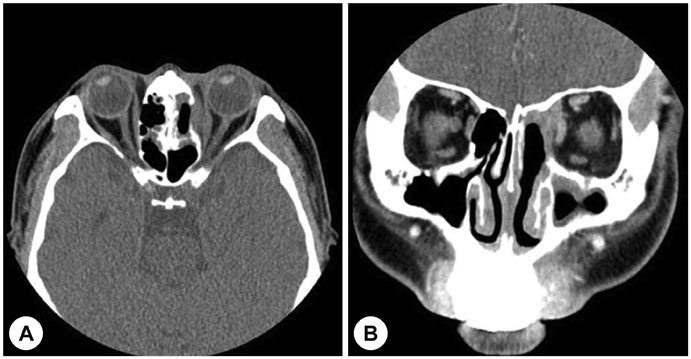
Fig. 4 Axial (A) and coronal (B) computerized tomography (CT) scans, performed 1 week after endoscopic removal of the retained wooden foreign body.
Reference
-
1. Banerjee A, Das A, Agarwal PK, Banerjee AR. Late spontaneous extrusion of a wooden intraorbital foreign body. Indian J Ophthalmol. 2003; 51(1):83–84.2. Al-Mujaini A, Al-Senawi R, Ganesh A, Al-Zuhaibi S, Al-Dhuhli H. Intraorbital foreign body: Clinical presentation, radiological appearance and management. Sultan Qaboos Univ Med J. 2008; 8(1):69–74.3. Lee DW, Jeong JS, Yoo SJ, Bae IH. A case of deep neck infection followed by orbital cellulitis. Korean J Otolaryngol-Head Neck Surg. 2006; 49(1):118–121.4. Lee JA, Lee HY. A case of retained wooden foreign body in orbit. Korean J Ophthalmol. 2002; 16(2):114–118.
Article5. Zenter J, Hassler W, Petersen D. A wooden foreign body penetrating the superior orbital fissure. Neurochirurgia. 1991; 34(6):188–190.
Article6. Miller CF, Brodkey JS, Colombi BJ. The danger of intracranial wood. Surg Neurol. 1977; 7(2):95–103.7. Shelsta HN, Bilyk JR, Rubin PA, Penne RB, Carrasco JR. Wooden intraorbital foreign body injuries: clinical characteristics and outcomes of 23 patients. Ophthal Plast Reconstr Surg. 2010; 26(4):238–244.
Article8. Kim YK, Kim KM, Woo HY. Two cases of sinogenic intracranial complications. Korean J Otolaryngol-Head Neck Surg. 1992; 35(4):578–583.9. Lagalla R, Manfre L, Caronia A, Bencivinni F, Duranti C, Ponte F. Plain film, CT and MRI sensibility in the evaluation of intraorbital foreign bodies in an in vitro model of the orbit and in pig eyes. Eur Radiol. 2000; 10(8):1338–1341.
Article10. Hansen JE, Gudeman SK, Holgate RC, Saunders RA. Penetrating intracranial wood wounds: Clinical limitations of computerized tomography. J Neurosurg. 1988; 68(5):752–756.
Article11. Boncoeur-Martel MP, Adenis JP, Rulfi JY, Robert PY, Dupuy JP, Maubon A. CT appearances of chronically retained wooden intraorbital foreign bodies. Neuroradiology. 2001; 43(2):165–168.
Article12. Karcioglu ZA, Nasr AM. Diagnosis and management of orbital inflammation and infections secondary to foreign bodies: a clinical review. Orbit. 1998; 17(4):247–269.
Article13. Glatt HJ, Custer PL, Barrett L, Sartor K. Magnetic resonance imaging and computed tomography in a model of wooden foreign bodies in the orbit. Ophthal Plast Reconstr Surg. 1990; 6(2):108–114.
Article
