Multiple Subretinal and Intraretinal Hemorrhages as a First Sign of Infective Endocarditis
- Affiliations
-
- 1Department of Ophthalmology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 2T2B Infrastructure Center for Ocular Disease, Inje University Busan Paik Hospital, Busan, Korea.
- 3Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. maekbak@hanmail.net
- KMID: 2397857
- DOI: http://doi.org/10.3341/jkos.2017.58.12.1416
Abstract
- PURPOSE
To report a patient with multiple subretinal and intraretinal hemorrhages in the absence of retinal/choroidal lesions, diagnosed with infective endocarditis (IE).
CASE SUMMARY
We describe the case of a 44-year-old male with an acute decrease of vision in his right eye. Ophthalmic evaluation revealed multiple subretinal and intraretinal hemorrhages, but no choroidal or other retinal lesions. A systemic examination revealed a pansystolic murmur and blood cultures with echocardiography were suggestive of IE.
CONCLUSIONS
Thorough systemic evaluations are important when patients present with subretinal and intraretinal hemorrhages in the absence of other retinal/choroidal lesions.
MeSH Terms
Figure
-
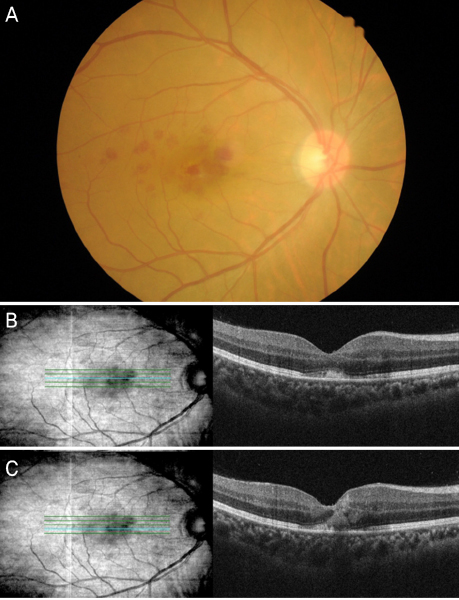
Figure 1 Fundus photograph and Optical coherence tomography images at the fist visit. (A) Fundus photograph of the right eye at the time of presentation. Multiple subretinal and intraretinal hemorrhages in the juxtafoveal area are apparent. Optical coherence tomography (OCT) images and red-free photographs of the right eye obtained at the time of presentation. Subretinal and intraretinal hemorrhages observed on OCT images corresponded with those on red-free photographs. (B) One line scan shows that the external limiting membrane (ELM) is intact, even though a hyper-reflective lesion is present between the ellipsoid zone and the retinal pigment epithelium layer. (C) A different line scan shows a disrupted ELM and hyper-reflective lesions that extend from the ganglion cell layer to the ellipsoid zone. The light blue line on the fundus shows the position at which the shown OCT line scan was obtained.
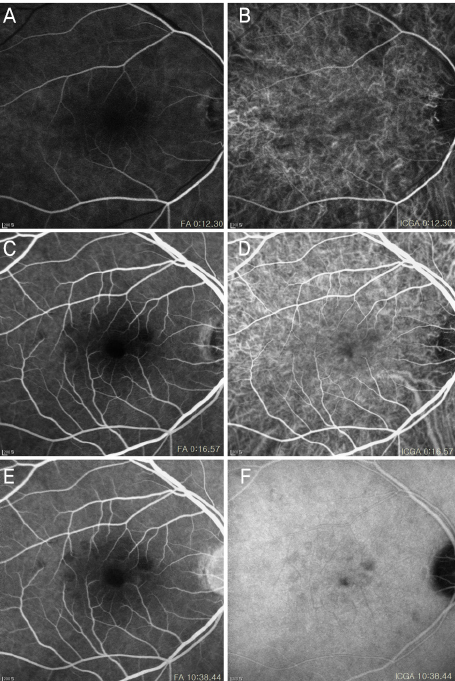
Figure 2 Fluorescein angiography (FA) and indocyanine green angiography (ICGA) images. (A, B) These images are arterial phase of FA and ICGA. (C-F) Both focal and round-shaped, juxtafoveal, hypofluorescent lesions are visible in venous phase and late phase. Hypofluroescent lesions indicate choroidal fluorescence blockage.

Figure 3 Transesophageal echocardiography showed multiple vegetations on the mitral valve (★). Accessory mitral valve leaflet prolapse (medial and middle portions) with severe eccentric mitral valve regurgitation (☆) was also apparent.
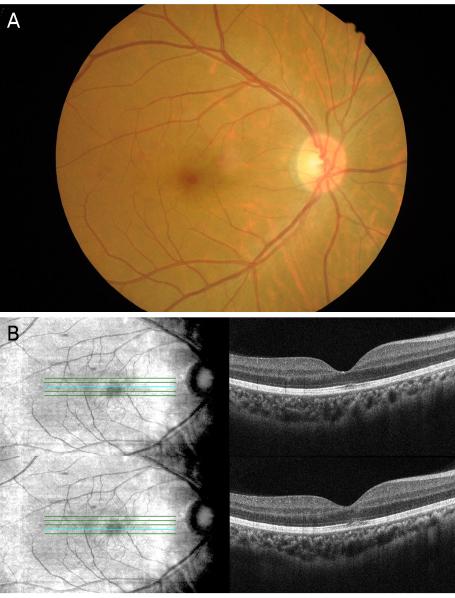
Figure 4 Ocular imaging obtained 1 month after the medical treatment. (A) The red-free photograph of the right eye shows a substantial decrease in hemorrhage size. (B) Optical coherence tomography (OCT) images showed only minor residual defects in the submacular ellipsoid and interdigitation zones. The light blue line on the fundus en face image shows the position at which the OCT line scan was obtained.
Reference
-
1. Hochman MA, Seery CM, Zarbin MA. Pathophysiology and management of subretinal hemorrhage. Surv Ophthalmol. 1997; 42:195–213.2. Silverman ME, Upshaw CB. Extracardiac manifestations of infective endocarditis andtheir historical descriptions. Am J Cardiol. 2007; 100:1802–1807.3. Walpot J, Klazen C, Blok W, van Zwienen J. Embolic events in infective endocarditis: a review and report of 4 cases. Acta Clin Belg. 2005; 60:139–145.4. Sandhya V, Shafquat S. Choroidal neovascularization (CNV) secondary to septic emboli from endocarditis: a case report. Eye (Lond). 2005; 19:822–823.5. Ling R, James B. White-centred retinal haemorrhages (Roth spots). Postgrad Med J. 1998; 74:581–582.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Infective Endocarditis Complicated with Multiple Myocotic Aneurysm and Mitral Valve Perforation
- Systemic Lupus Erythematosus with Purtscher-Like Retinopathy as the First Symptom
- Macroaneurysms of Retinal Arteries
- Neurologic Complications of Infective Endocarditis:Retrospective Review of 100 Cases
- A case of Libman-Sacks endocarditis confused with infective endocarditis
