The Efficacy of Fibroblast Growth Factor for the Treatment of Chronic Vocal Fold Scarring: From Animal Model to Clinical Application
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Cheonan, Korea.
- 2Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Seoul, Korea.
- 3Department of Otolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea. lsw0922@schmc.ac.kr
- 4Department of Pathology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- KMID: 2396791
- DOI: http://doi.org/10.21053/ceo.2016.00941
Abstract
OBJECTIVES
This study assessed the regenerative efficacy of basic fibroblast growth factor (FGF) in a rabbit model of chronic vocal fold scarring and then confirmed its utility and safety in a prospective trial of patients with this condition.
METHODS
FGF was injected three times, at 1-week intervals, into a chronic vocal fold scar created in a rabbit model. After 1 month, mRNA level of procollagen I, hyaluronic acid synthetase 2 (HAS 2), and matrix metalloproteinase 2 (MMP 2) were analyzed by real-time polymerase chain reaction. The relative densities of hyaluronic acid (HA) and collagen were examined 3 months post-injection. From April 2012 to September 2014, a prospective clinical trial was conducted at a tertiary hospital in Korea. FGF was injected into the mild vocal fold scar of 17 consecutive patients with a small glottic gap. The patients underwent perceptual, stroboscopic, acoustic aerodynamic test, and Voice Handicap Index (VHI) survey prior to and 3, 6, and 12 months after FGF injection.
RESULTS
FGF injection of the vocal fold scar decreased the density of collagen and increased mRNA level of HAS 2 and MMP 2 expression significantly compared to the control group injected with phosphate buffered solution in a rabbit model (P < 0.05). In the clinical trial, significant improvements in the majority of the subjective and objective voice parameters were registered 3 months after FGF injection and were maintained at 12 months. Complications associated with the FGF injections, such as granuloma, were not observed during the follow-up period.
CONCLUSION
Based on the animal model and the prospective clinical trial, vocal fold injections of FGF in patients with mild chronic vocal fold scarring can significantly improve voice quality for as long as 1 year and without side effects. Our results recommend the use of FGF vocal fold injection as an alternative treatment modality for mild chronic vocal fold scarring.
Keyword
MeSH Terms
-
Acoustics
Animals*
Cicatrix*
Collagen
Dysphonia
Fibroblast Growth Factor 2
Fibroblast Growth Factors*
Fibroblasts*
Follow-Up Studies
Granuloma
Humans
Hyaluronic Acid
Korea
Ligases
Matrix Metalloproteinase 2
Models, Animal*
Procollagen
Prospective Studies
Real-Time Polymerase Chain Reaction
RNA, Messenger
Specific Gravity
Tertiary Care Centers
Vocal Cords*
Voice
Voice Quality
Collagen
Fibroblast Growth Factor 2
Fibroblast Growth Factors
Hyaluronic Acid
Ligases
Matrix Metalloproteinase 2
Procollagen
RNA, Messenger
Figure
-
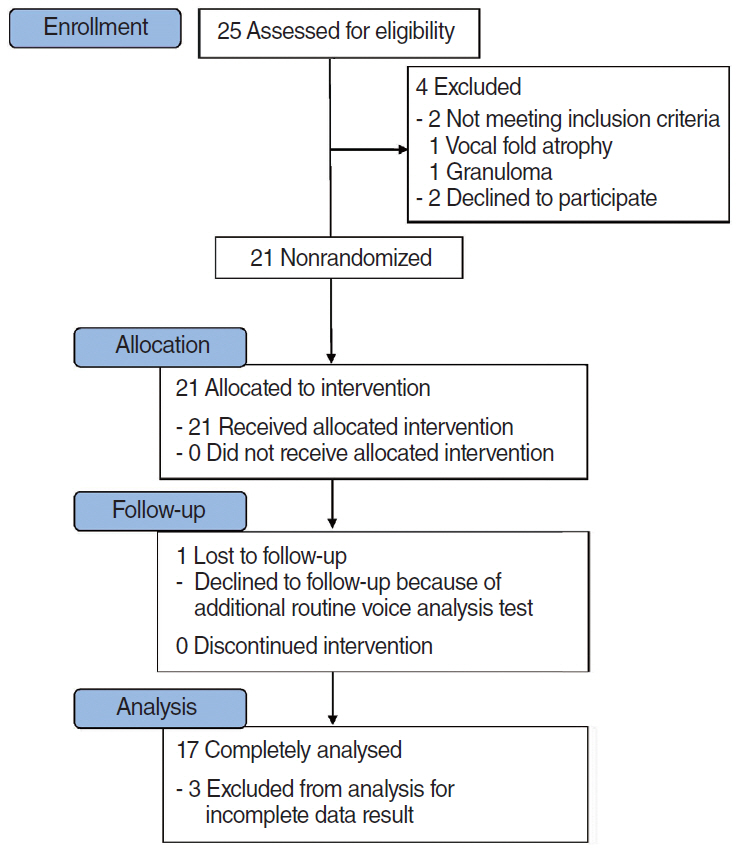
Fig. 1. Consort flow diagram. A common reason for declining trial participation at enrollment and follow-up was that long travel distances made patients unwilling to return to the hospital for the 1-year follow-up visit. Chronic vocal fold scar is a clinical diagnosis, and 2 patients were found at stroboscopy to have vocal fold disease where fibroblast growth factor injection is not indicated. Three patients were excluded for incomplete voice evaluation data result.
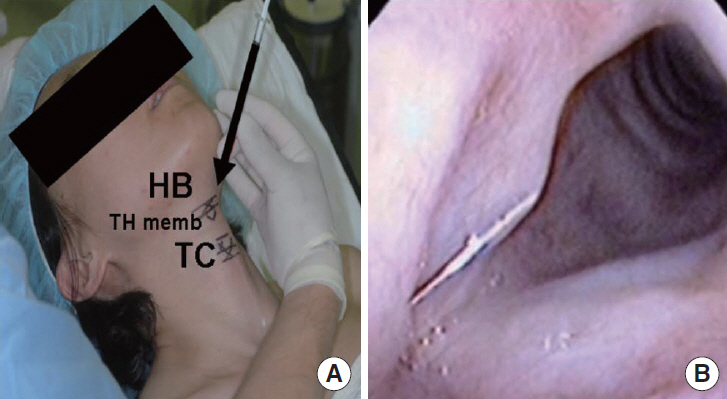
Fig. 2. Injection of fibroblast growth factor into lamina propria of chronic vocal fold under local anesthesia. (A) Surgical photograph of procedure and (B) fiberoscopic view of injection. HB, hyoid bone; TH memb, thyrohyoid membrane; TC, thyroid cartilage.

Fig. 3. Normalized mRNA expression ratios of procollagen type I, hyaluronic acid synthase 2 (HAS 2), and matrix metalloproteinase 2 (MMP 2). The results are expressed as the fold change in target gene mRNA expression relative to mRNA expression of the housekeeping gene, β-actin. Each sample was tested in duplicate. HAS 2 and MMP 2 expression increased significantly in the FGF-injected group vs. PBS-injected group. The error bars represent the 95% confidence intervals of the mean. FGF, fibroblast growth factor; PBS, phosphate-buffered saline. *P<0.05 in a Mann-Whitney U-test.
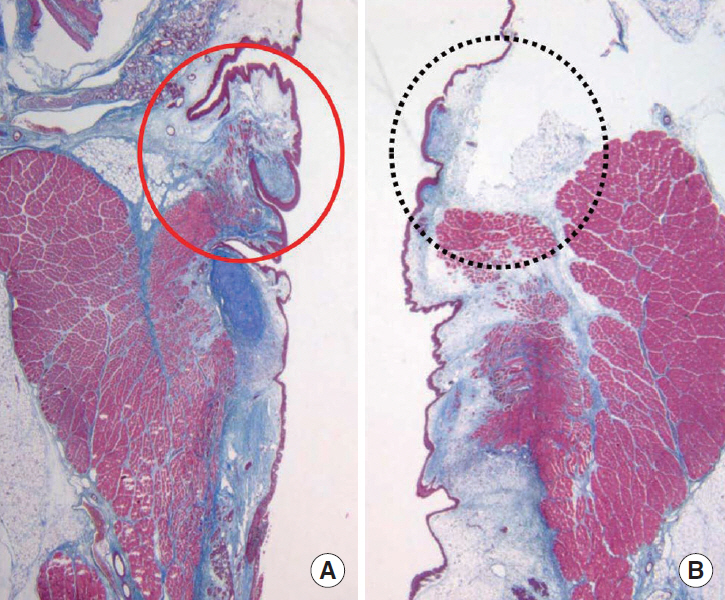
Fig. 4. Masson’s trichrome staining of the vocal folds injected with (A) phosphate-buffered saline (PBS; 0.1 mL) and (B) fibroblast growth factor (FGF; 10 μg / 0.1 mL). Injection was performed 3 months after the scar-inducing injury. Coronal sections (6-μm thick) were prepared from the laryngeal tissues of 12 rabbits euthanized 6 months after scar formation. The FGF-injected fold (black dotted circle) shows greater vocal fold volume without an increase in the density of blue stained collagen (×20) than PBS-injected fold (red circle).

Fig. 5. Histological image analysis of hyaluronic acid (HA) and relative collagen density in the FGF-injected group vs. the PBS-injected group. The relative density of collagen was significantly lower whereas that of HA was not significantly higher in the FGF-injected group vs. PBS-injected groups. FGF, fibroblast growth factor; PBS, phosphate-buffered saline. *P<0.05 in a Mann-Whitney U-test.
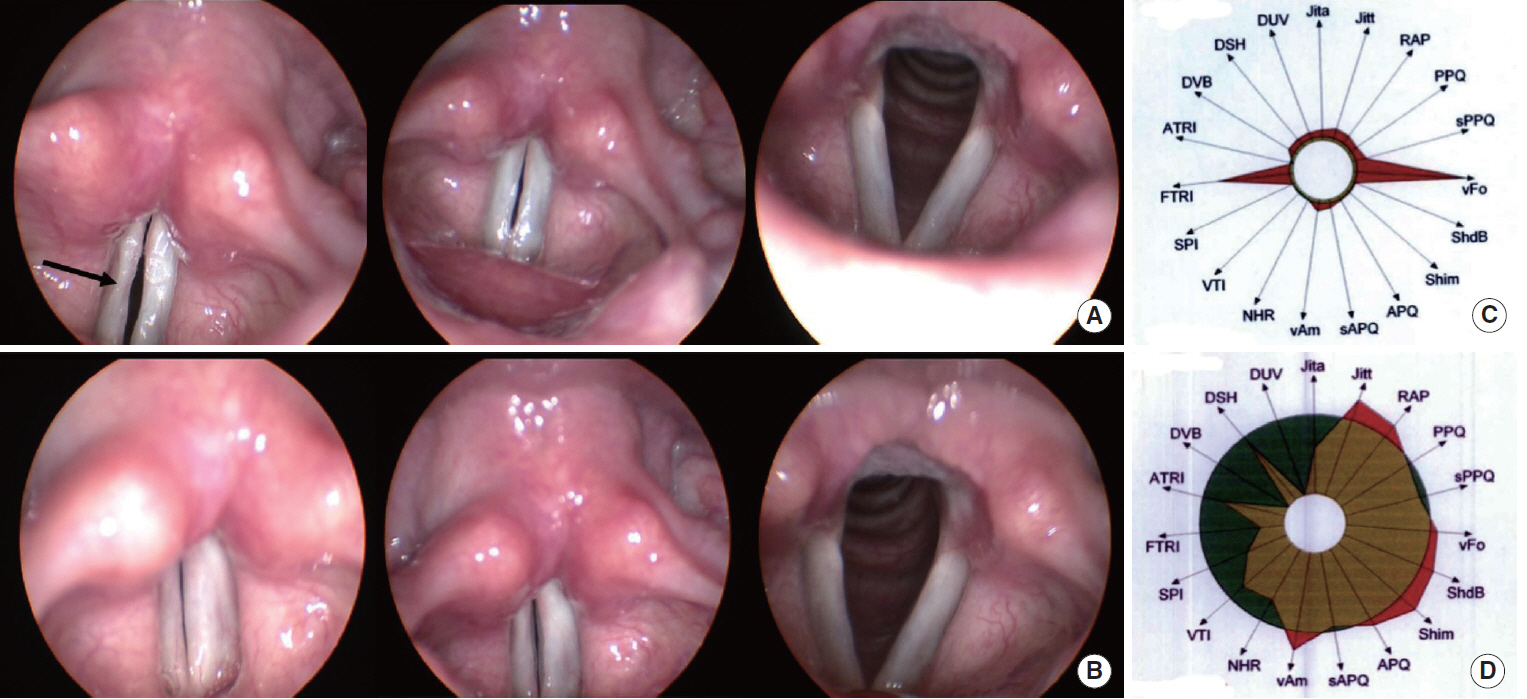
Fig. 6. Representative stroboscopic findings and Multi-Dimensional Voice Program (MDVP) diagrams of a patient who received fibroblast growth factor (FGF) injection. (A) Preoperative findings, demonstrating a chronic vocal focal scar with minimal glottis gap on the right vocal fold that impairs mucosal vibration (Glottal closure grade 2, Mucosal wave grade 1). The arrow highlights the scar. (B) 12 Months after injection. Vocal scar disappeared resulting in complete glottal closure and improved glottal vibratory function (Glottal closure grade 3, Mucosal wave grade 3). Glottal closure and the mucosal wave were graded on a four-point scale. 0=severe glottis gap, no wave; 1=moderate glottis gap, obvious decreased mucosal wave; 2=mild glottis gap, slightly decreased mucosal wave; and 3=complete closure, full wave. Before (C) and after (D) FGF injection, the MDVP diagram showed improved objective voice parameters including Jitt, Shim, and NHR. Jita, absolute jitter (μs); Jitt, jitter percent (%); RAP, relative average perturbation (%); PPQ, pitch perturbation quotient (%); sPPQ, smoothed pitch perturbation quotient (%); vF0, fundamental frequency variation (%); ShdB, shimmer in dB (dB); Shim, shimmer percent (%); APQ, amplitude perturbation quotient (%); sAPQ, smoothed amplitude perturbation quotient (%); vAm, peak-amplitude variation (%); NHR, noise to harmonic ratio; VTI, Voice Turbulence Index; SPI, Soft Phonation Index; FTRI, F0-Tremor Intensity Index (%); ATRI, Amplitude Tremor Intensity Index (%); DVB, degree of voice breaks (%); DSH, degree of sub-harmonics (%); DUV, degree of voiceless (%).
Reference
-
1. Hirano S. Current treatment of vocal fold scarring. Curr Opin Otolaryngol Head Neck Surg. 2005; Jun. 13(3):143–7.
Article2. Suehiro A, Hirano S, Kishimoto Y, Rousseau B, Nakamura T, Ito J. Treatment of acute vocal fold scar with local injection of basic fibroblast growth factor: a canine study. Acta Otolaryngol. 2010; Jul. 130(7):844–50.
Article3. Rousseau B, Hirano S, Chan RW, Welham NV, Thibeault SL, Ford CN, et al. Characterization of chronic vocal fold scarring in a rabbit model. J Voice. 2004; Mar. 18(1):116–24.
Article4. Lim JY, Choi BH, Lee S, Jang YH, Choi JS, Kim YM. Regulation of wound healing by granulocyte-macrophage colony-stimulating factor after vocal fold injury. PLoS One. 2013; 8(1):e54256.
Article5. Lee SW, Kim JW, Lee JY, Chang HS, Kim HK, Choi EC. Augmentation of vocal fold using a fat block implant following cordotomy through a minithyrotomy approach in a rabbit model. J Voice. 2012; Jul. 26(4):521–5.
Article6. Hirano M. Clinical examination of voice. Wien: Springer-Verlag;1981.7. Yun YS, Kim HH, Son YI, Choi HS. Validation of the Korean Voice Handicap Index (K-VHI) and the clinical usefulness of Korean VHI-10. Korean J Commun Disord. 2008; Jun. 13(2):216–41.8. Lee SW, Kim JW, Koh YW, Shim SS, Son YI. Comparative analysis of efficiency of injection laryngoplasty technique for with or without neck treatment patients: a transcartilaginous approach versus the cricothyroid approach. Clin Exp Otorhinolaryngol. 2010; Mar. 3(1):37–41.
Article9. Yoon KC, Mun GH, Kim SD, Kim SH, Kim CY, Park KH, et al. Prevalence of eye diseases in South Korea: data from the Korea National Health and Nutrition Examination Survey 2008-2009. Korean J Ophthalmol. 2011; Dec. 25(6):421–33.
Article10. Hirano S, Minamiguchi S, Yamashita M, Ohno T, Kanemaru S, Kitamura M. Histologic characterization of human scarred vocal folds. J Voice. 2009; Jul. 23(4):399–407.
Article11. Dailey SH, Ford CN. Surgical management of sulcus vocalis and vocal fold scarring. Otolaryngol Clin North Am. 2006; Feb. 39(1):23–42.
Article12. Kanemaru S, Nakamura T, Omori K, Kojima H, Magrufov A, Hiratsuka Y, et al. Regeneration of the vocal fold using autologous mesenchymal stem cells. Ann Otol Rhinol Laryngol. 2003; Nov. 112(11):915–20.
Article13. Hirano S, Bless D, Heisey D, Ford C. Roles of hepatocyte growth factor and transforming growth factor beta1 in production of extracellular matrix by canine vocal fold fibroblasts. Laryngoscope. 2003; Jan. 113(1):144–8.14. Hirano S, Bless DM, Heisey D, Ford CN. Effect of growth factors on hyaluronan production by canine vocal fold fibroblasts. Ann Otol Rhinol Laryngol. 2003; Jul. 112(7):617–24.
Article15. Hirano S, Bless DM, Rousseau B, Welham N, Montequin D, Chan RW, et al. Prevention of vocal fold scarring by topical injection of hepatocyte growth factor in a rabbit model. Laryngoscope. 2004; Mar. 114(3):548–56.
Article16. Hirano S, Bless DM, Nagai H, Rousseau B, Welham NV, Montequin DW, et al. Growth factor therapy for vocal fold scarring in a canine model. Ann Otol Rhinol Laryngol. 2004; Oct. 113(10):777–85.
Article17. Ohno T, Hirano S, Kanemaru S, Yamashita M, Umeda H, Suehiro A, et al. Drug delivery system of hepatocyte growth factor for the treatment of vocal fold scarring in a canine model. Ann Otol Rhinol Laryngol. 2007; Oct. 116(10):762–9.
Article18. Hirano S, Mizuta M, Kaneko M, Tateya I, Kanemaru SI, Ito J. Regenerative phonosurgical treatments for vocal fold scar and sulcus with basic fibroblast growth factor. Laryngoscope. 2013; Nov. 123(11):2749–55.
Article19. Hong HH, Trackman PC. Cytokine regulation of gingival fibroblast lysyl oxidase, collagen, and elastin. J Periodontol. 2002; Feb. 73(2):145–52.
Article20. Heldin P, Laurent TC, Heldin CH. Effect of growth factors on hyaluronan synthesis in cultured human fibroblasts. Biochem J. 1989; Mar. 258(3):919–22.
Article21. Kanazawa T, Komazawa D, Indo K, Akagi Y, Lee Y, Nakamura K, et al. Single injection of basic fibroblast growth factor to treat severe vocal fold lesions and vocal fold paralysis. Laryngoscope. 2015; Oct. 125(1):E338–44.
Article22. Tateya T, Tateya I, Bless DM. Immuno-scanning electron microscopy of collagen types I and III in human vocal fold lamina propria. Ann Otol Rhinol Laryngol. 2007; Feb. 116(2):156–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histological Effect of Basic Fibroblast Growth Factor on Chronic Vocal Fold Scarring in a Rat Model
- A Case of Surgical Treatment of Intractable Vocal Fold Scar Using Basic Fibroblast Growth Factor and Collagen Scaffold
- Vocal Fold Injection: Review of Indications, Techniques, and Materials for Augmentation
- Vocal Fold Regeneration: Current Review
- The Study of Bilateral Venign Vocal Fold Lesions
