Juxtacortical Osteoma of the Metatarsal Bone: A Case Report
- Affiliations
-
- 1Department of Radiology, Sungkyunkwan University School of Medicine, Kangbuk Samsung Hospital, Seoul, Korea. parkhiji@gmail.com
- KMID: 2396502
- DOI: http://doi.org/10.3348/jksr.2017.77.6.421
Abstract
- Osteoma is a benign bone-forming tumor composed of compact or mature trabecular bone and is limited almost exclusively to craniofacial bones, especially in the paranasal sinuses and mandible. It is typically a slow growing lesion that is asymptomatic, unless its size significantly increases to cause symptoms such as pain or other neurological symptoms, that happens more often in cases involving craniofacial bones. Radiological appearance of these tumors depends on their location. In cases of juxtacortical osteoma, it is crucial to differentiate between this type of tumor and parosteal osteosarcoma, sessile osteochondroma, and matured juxtacortical focus of myositis ossificans. However, in some cases, it is difficult to differentiate juxtacortical osteoma from above mentioned lesions only with radiologic appearance. We describe a case of an osteoma that arose from the second metatarsal bone, a rare anatomical location for osteoma.
MeSH Terms
Figure
-
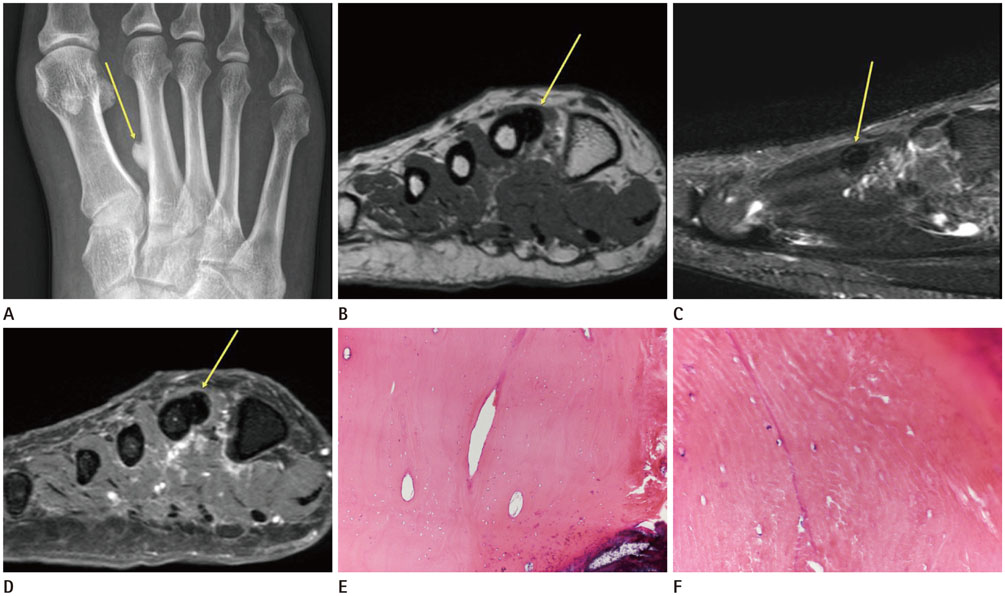
Fig. 1 Juxtacortical osteoma arising from the second metatarsal bone in a 61-year-old woman. A. Anterior-posterior plain radiograph of the right foot showing a small, well-demarcated, exophytic, sessile, calcified mass in the shaft of the second metatarsal bone (arrow). B-D. MR images of the second metatarsal bone. MR images reveal that the lesion has the same signal intensity as the cortical bone and reveals no cartilaginous cap. On coronal T1-weighted image (TR = 600, TE = 15) and sagittal, fat-suppressed, T2-weighted image (TR = 6000, TE = 100), the lesion is homogeneously hypointense (B, C, arrows). Contrast-enhanced, fat-suppressed T1-weighted image (TR = 600, TE = 15) reveal no enhancement (D, arrow). E, F. Histopathology revealing that the tissue consists of mature lamellar bone with multiple osteocytes in lacuna [E (H&E stain, × 100) and F (H&E stain, × 400)]. H&E = hematoxylin and eosin, MR = magnetic resonance, TE = echo time, TR = repetition time
Reference
-
1. McHugh JB, Mukherji SK, Lucas DR. Sino-orbital osteoma: a clinicopathologic study of 45 surgically treated cases with emphasis on tumors with osteoblastoma-like features. Arch Pathol Lab Med. 2009; 133:1587–1593.2. Bertoni F, Unni KK, Beabout JW, Sim FH. Parosteal osteoma of bones other than of the skull and face. Cancer. 1995; 75:2466–2473.3. Gümüştaş S, Aǵır İ, Tosun HB, İnan HM. An osteoma located on the radial head: a case report. J Clin Anal Med. 2013; 4:Suppl 3. 269–271.4. Lambiase RE, Levine SM, Terek RM, Wyman JJ. Long bone surface osteomas: imaging features that may help avoid unnecessary biopsies. AJR Am J Roentgenol. 1998; 171:775–778.5. O'Connell JX, Rosenthal DI, Mankin HJ, Rosenberg AE. Solitary osteoma of a long bone. A case report. J Bone Joint Surg Am. 1993; 75:1830–1834.6. Greenspan A. Benign bone-forming lesions: osteoma, osteoid osteoma, and osteoblastoma. Clinical, imaging, pathologic, and differential considerations. Skeletal Radiol. 1993; 22:485–500.7. Baum PA, Nelson MC, Lack EE, Bogumill GP. Case report 560: parosteal osteoma of tibia. Skeletal Radiol. 1989; 18:406–409.8. Lee JK, Yao L, Wirth CR. MR imaging of solitary osteochondromas: report of eight cases. AJR Am J Roentgenol. 1987; 149:557–560.9. Inokuchi T, Hitora T, Yamagami Y, Nishimura H, Yamamoto T. Parosteal osteoma of the clavicle. Case Rep Orthop. 2014; 2014:824959.10. Murphey MD, Jelinek JS, Temple HT, Flemming DJ, Gannon FH. Imaging of periosteal osteosarcoma: radiologic-pathologic comparison. Radiology. 2004; 233:129–138.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Case Report of Recurrent Osteoma at the Grafted Bone
- Juxtacortical chondromyxoid fibroma in the small bones: two cases with unusual location and a literature review
- A Case of Osteoma Originated from the Squama of Temporal Bone
- Stress Fracture on the 4th Metatarsal Bone after Treatment of Stress Fracture on the 5th Metatarsal Bone: A Case Report
- Osteoid Osteoma of the patella: a case report
