Local recurrence and subsequent endoscopic treatment after endoscopic piecemeal mucosal resection with or without precutting in the colorectum
- Affiliations
-
- 1Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jsbyeon@amc.seoul.kr
- KMID: 2396400
- DOI: http://doi.org/10.5217/ir.2017.15.4.502
Abstract
- BACKGROUND/AIMS
Precutting before endoscopic piecemeal mucosal resection (EPMR) may increase colorectal polyp resection effectiveness. We aimed to identify risk factors for recurrence after conventional EPMR (CEPMR) and precut EPMR (PEPMR) and investigated endoscopic treatment outcomes for recurrent cases.
METHODS
The medical records of patients with colorectal polyps treated by EPMR were analyzed. Patients without follow-up surveillance colonoscopies were excluded.
RESULTS
Among 359 lesions, the local recurrence rate on the first surveillance colonoscopy was 5.8% (18/312) and 6.4% (3/47) after CEPMR and PEPMR, respectively. Among lesions without recurrence at the first surveillance colonoscopy, the rates of late recurrence on subsequent surveillance colonoscopy were 3.9% (6/152) and 0% after CEPMR and PEPMR, respectively. Larger tumor size was the only independent risk factor for recurrence (odds ratio, 7.93; 95% confidence interval, 1.95-32.30; P<0.001). Endoscopic treatment was performed for all 27 recurrences. A combination of ≥2 endoscopic treatment modalities was used in 19 of 27 recurrences (70.4%). Surveillance colonoscopies were performed in 20 of 27 recurrences after endoscopic treatment. One (5.0%) had a re-recurrence and was treated by surgical resection because recurrence occurred at the appendiceal orifice. Nineteen of 20 lesions (95.0%) could be cured endoscopically, although 3 of the 19 showed second or third recurrences and were treated by repeat endoscopic resection.
CONCLUSIONS
The local recurrence rates after CEPMR and PEPMR were similar. Larger tumor size was an independent risk factor for local recurrence after EPMR. Endoscopic treatment of recurrences resulted in high cure rates, although combination methods were necessary in many cases.
Figure
-
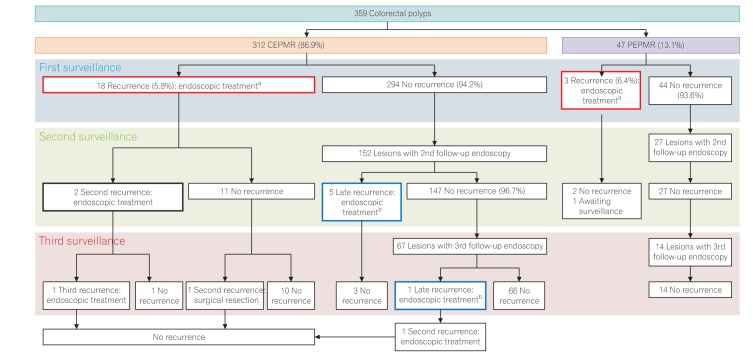
Fig. 1 Flow diagram showing recurrence and subsequent endoscopic treatment. aEarly recurrence (red box) rates at the first surveillance were 5.8% (18/312) and 6.4% (3/47) after conventional endoscopic piecemeal mucosal resection (CEPMR) and precut EPMR (PEPMR), respectively; bAmong lesions without recurrence at the first surveillance colonoscopy, the rates of late recurrence (blue box) were 3.9% (6/152) and 0% after CEPMR and PEPMR, respectively. In summary, the overall recurrence rates were 7.7% (24/312) and 6.4% (3/47) after CEPMR and PEPMR, respectively.
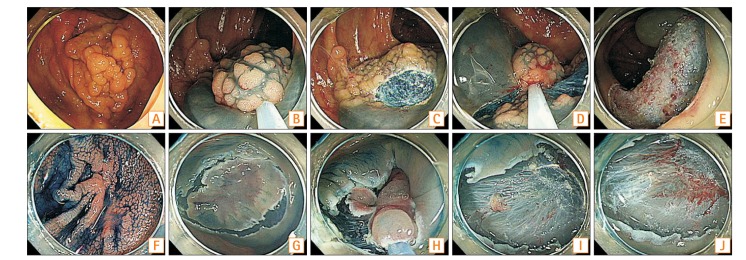
Fig. 2 Conventional endoscopic piecemeal resection (EPMR) (A-E) and precut EPMR (F-J).
Cited by 1 articles
-
Clinical outcomes of submucosal colorectal cancer diagnosed after endoscopic resection: a focus on the need for surgery
Yun Sik Choi, Wan Soo Kim, Sung Wook Hwang, Sang Hyoung Park, Dong-Hoon Yang, Byong Duk Ye, Seung-Jae Myung, Suk-Kyun Yang, Jeong-Sik Byeon
Intest Res. 2020;18(1):96-106. doi: 10.5217/ir.2019.00092.
Reference
-
1. Moss A, Williams SJ, Hourigan LF, et al. Long-term adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut. 2015; 64:57–65. PMID: 24986245.
Article2. Khashab M, Eid E, Rusche M, Rex DK. Incidence and predictors of “late” recurrences after endoscopic piecemeal resection of large sessile adenomas. Gastrointest Endosc. 2009; 70:344–349. PMID: 19249767.
Article3. Oka S, Tanaka S, Saito Y, et al. Local recurrence after endoscopic resection for large colorectal neoplasia: a multicenter prospective study in Japan. Am J Gastroenterol. 2015; 110:697–707. PMID: 25848926.
Article4. Tanaka S, Haruma K, Oka S, et al. Clinicopathologic features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc. 2001; 54:62–66. PMID: 11427843.
Article5. Yang DH, Jeong GH, Song Y, et al. The feasibility of performing colorectal endoscopic submucosal dissection without previous experience in performing gastric endoscopic submucosal dissection. Dig Dis Sci. 2015; 60:3431–3441. PMID: 26088371.
Article6. Woodward TA, Heckman MG, Cleveland P, De Melo S, Raimondo M, Wallace M. Predictors of complete endoscopic mucosal resection of flat and depressed gastrointestinal neoplasia of the colon. Am J Gastroenterol. 2012; 107:650–654. PMID: 22552236.
Article7. Saito Y, Fukuzawa M, Matsuda T, et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surg Endosc. 2010; 24:343–352. PMID: 19517168.
Article8. Lee EJ, Lee JB, Lee SH, Youk EG. Endoscopic treatment of large colorectal tumors: comparison of endoscopic mucosal resection, endoscopic mucosal resection-precutting, and endoscopic submucosal dissection. Surg Endosc. 2012; 26:2220–2230. PMID: 22278105.
Article9. Tajika M, Niwa Y, Bhatia V, et al. Comparison of endoscopic submucosal dissection and endoscopic mucosal resection for large colorectal tumors. Eur J Gastroenterol Hepatol. 2011; 23:1042–1049. PMID: 21869682.
Article10. Byeon JS, Yang DH, Kim KJ, et al. Endoscopic submucosal dissection with or without snaring for colorectal neoplasms. Gastrointest Endosc. 2011; 74:1075–1083. PMID: 21663905.11. Hong YM, Kim HW, Park SB, Choi CW, Kang DH. Endoscopic mucosal resection with circumferential incision for the treatment of large sessile polyps and laterally spreading tumors of the colorectum. Clin Endosc. 2015; 48:52–58. PMID: 25674527.12. Sakamoto T, Matsuda T, Nakajima T, Saito Y. Efficacy of endoscopic mucosal resection with circumferential incision for patients with large colorectal tumors. Clin Gastroenterol Hepatol. 2012; 10:22–26. PMID: 22016034.13. Kim HG, Sethi S, Banerjee S, Friedland S. Outcomes of endoscopic treatment of second recurrences of large nonpedunculated colorectal adenomas. Surg Endosc. 2016; 30:2457–2464. PMID: 26423413.14. Sakamoto T, Saito Y, Matsuda T, Fukunaga S, Nakajima T, Fujii T. Treatment strategy for recurrent or residual colorectal tumors after endoscopic resection. Surg Endosc. 2011; 25:255–260. PMID: 20559661.15. Schlemper RJ, Riddell RH, Kato Y, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut. 2000; 47:251–255. PMID: 10896917.
Article16. Seo GJ, Sohn DK, Han KS, et al. Recurrence after endoscopic piecemeal mucosal resection for large sessile colorectal polyps. World J Gastroenterol. 2010; 16:2806–2811. PMID: 20533602.
Article17. Hotta K, Fujii T, Saito Y, Matsuda T. Local recurrence after endoscopic resection of colorectal tumors. Int J Colorectal Dis. 2009; 24:225–230. PMID: 18972121.
Article18. Belderbos TD, Leenders M, Moons LM, Siersema PD. Local recurrence after endoscopic mucosal resection of nonpedunculated colorectal lesions: systematic review and meta-analysis. Endoscopy. 2014; 46:388–402. PMID: 24671869.
Article19. Sakamoto T, Matsuda T, Otake Y, Nakajima T, Saito Y. Predictive factors of local recurrence after endoscopic piecemeal mucosal resection. J Gastroenterol. 2012; 47:635–640. PMID: 22223177.
Article20. Regula J, Wronska E, Polkowski M, et al. Argon plasma coagulation after piecemeal polypectomy of sessile colorectal adenomas: long-term follow-up study. Endoscopy. 2003; 35:212–218. PMID: 12584639.
Article21. Tsiamoulos ZP, Bourikas LA, Saunders BP. Endoscopic mucosal ablation: a new argon plasma coagulation/injection technique to assist complete resection of recurrent, fibrotic colon polyps (with video). Gastrointest Endosc. 2012; 75:400–404. PMID: 22154411.
Article22. Holmes I, Kim HG, Yang DH, Friedland S. Avulsion is superior to argon plasma coagulation for treatment of visible residual neoplasia during EMR of colorectal polyps (with videos). Gastrointest Endosc. 2016; 84:822–829. PMID: 27080417.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrence after endoscopic resection of small rectal neuroendocrine tumors: a retrospective cohort study
- Repeatedly Recurrent Colon Cancer Involving the Appendiceal Orifice after Endoscopic Piecemeal Mucosal Resection: A Case Report
- Efficacy and Safety of Complete Endoscopic Resection of Colorectal Neoplasia Using a Stepwise Endoscopic Protocol with SOUTEN, a Novel Multifunctional Snare
- Re-Endoscopic Mucosal Resection for a Residual or Locally Recurrent Gastric Lesion after Endoscopic Mucosal Resection
- Comparison of Endoscopic Submucosal Dissection With Endoscopic Mucosal Resection After Circumferential Precutting to Treat Gastric Adenomas ≤15 mm
