The First Successful Lung Transplantation in a Korean Child with Cystic Fibrosis
- Affiliations
-
- 1Department of Pediatrics, Childhood Asthma Atopy Center, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. sjhong@amc.seoul.kr
- 2Department of Pediatrics, Chonnam National University Hospital, Gwangju, Korea.
- 3Environmental Health Center, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 4Department of Pediatrics, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- KMID: 2396389
- DOI: http://doi.org/10.3346/jkms.2017.32.12.2073
Abstract
- Cystic fibrosis (CF) is an autosomal recessive inherited multisystem disorder caused by mutations of the gene encoding the cystic fibrosis transmembrane conductance regulator (CFTR) protein. Respiratory failure remains the most frequent cause of morbidity and mortality. Lung transplantation is the only option to treat end-stage lung disease. Very few cases of CF occur in Koreans. We report the case of a 12-year-old girl with respiratory failure due to CF who underwent lung transplantation. She had been diagnosed with CF 8 years previously after being treated for recurrent Pseudomonas aeruginosa pneumonia and malnutrition based on sweat chloride concentrations and the CFTR protein gene mutation test. Progression to end-stage lung disease and respiratory failure led to registration with the Korean Network for Organ Sharing. She underwent successful double lung transplantation in 2014. Although she has diabetes mellitus and chronic kidney disease, she has a better quality of life and a prolonged life expectancy.
Keyword
MeSH Terms
-
Child*
Cystic Fibrosis Transmembrane Conductance Regulator
Cystic Fibrosis*
Diabetes Mellitus
Female
Humans
Korea
Life Expectancy
Lung Diseases
Lung Transplantation*
Lung*
Malnutrition
Mortality
Pneumonia
Pseudomonas aeruginosa
Quality of Life
Renal Insufficiency, Chronic
Respiratory Insufficiency
Sweat
Cystic Fibrosis Transmembrane Conductance Regulator
Figure
-
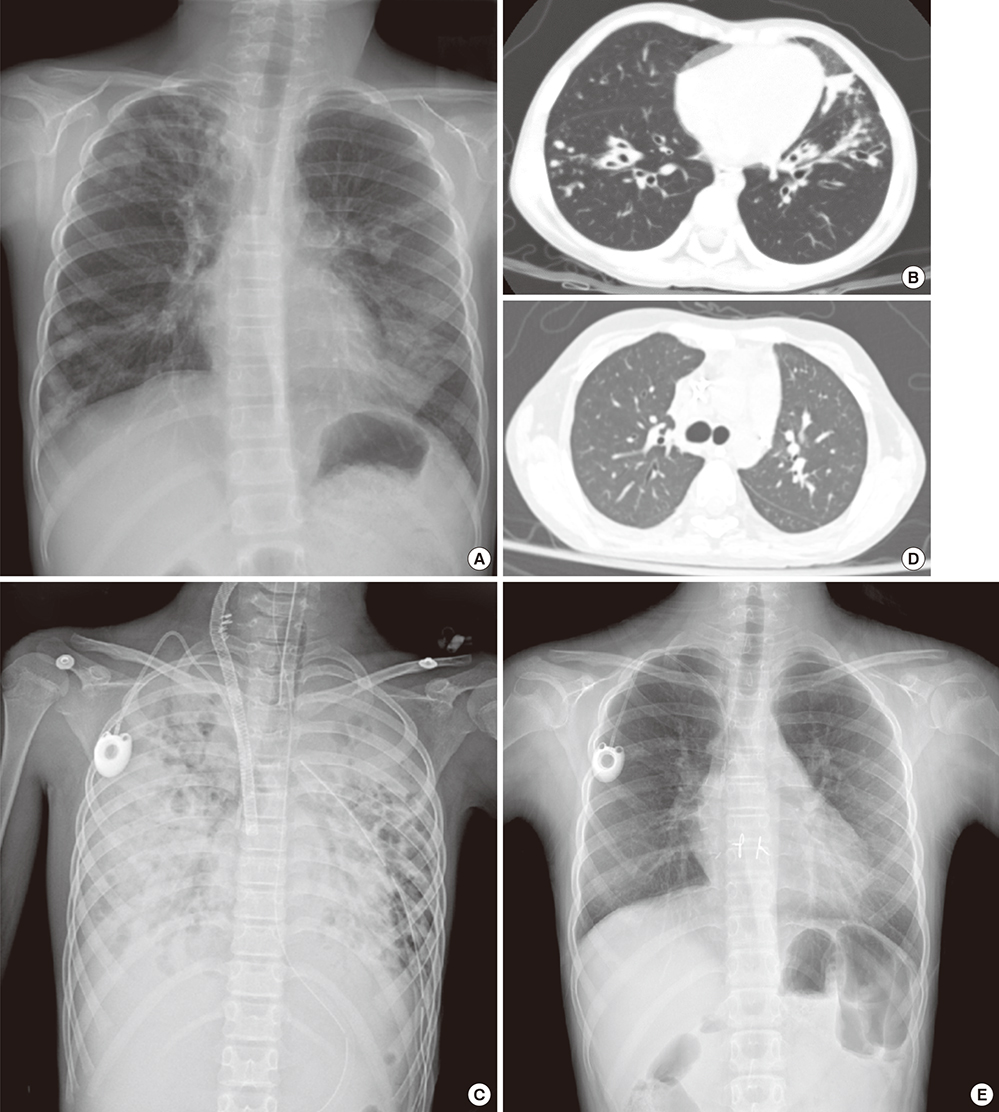
Fig. 1 Serial follow-up of radiologic findings before and after lung transplantation. (A) Initial chest X-ray at first admission to our hospital showing bronchiectasis and multifocal nodular opacity with peribronchial infiltration in both lungs (at the age of 7 years). (B) Chest CT scan taken at first admission showing bronchiectasis and consolidation in the right upper lobe and anterior basal segment of the left lower lobe (at the age of 7 years). (C) Chest X-ray taken one day before lung transplantation showing an increased extent of consolidation in both lungs. At that time, saturation was not maintained at 100% oxygen via a ventilator and ECMO (SpO2 75%–80%, pO2 35–40). (D) Follow-up chest CT scan taken 5 months after lung transplantation. (E) Follow-up chest X-ray at 2 years and 6 months after lung transplantation showing no remarkable findings. CT = computed tomography, ECMO = extracorporeal membrane oxygenation.
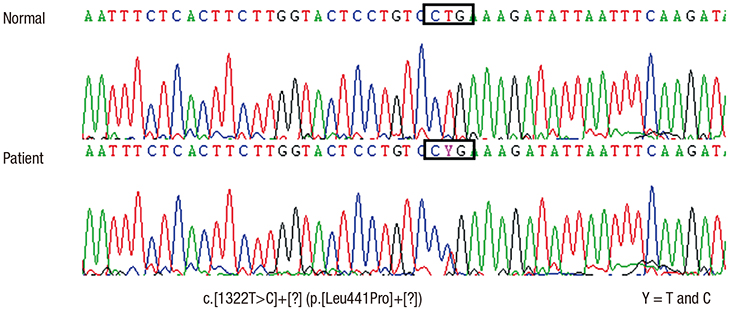
Fig. 2 Genotyping of CFTR. A heterozygous T to C transition was identified (c.1322T>C), but mutation of the opposite allele was not detectable. CFTR = cystic fibrosis transmembrane conductance regulator.
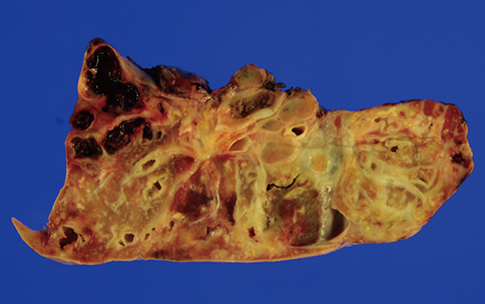
Fig. 3 Gross findings of the explanted lung of the recipient showing dilated bronchioles and diffuse fibrotic lung parenchyma with atrophy.
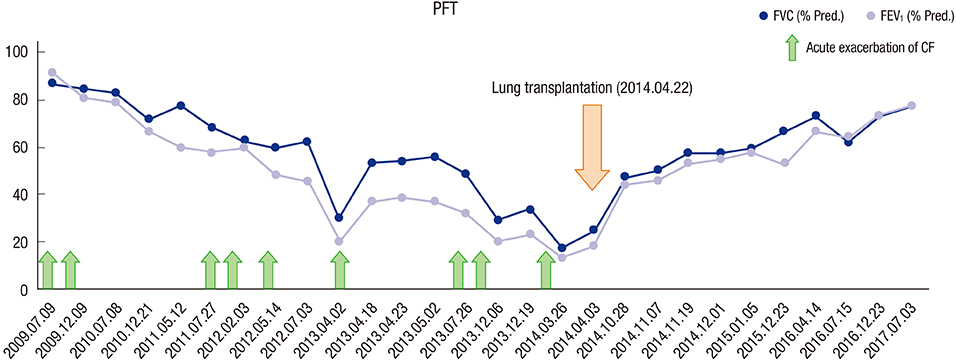
Fig. 4 Graph of the PFTs. After the lung transplantation, FVC and FEV1 gradually improved. PFT = pulmonary function test, FVC = forced vital capacity, FEV1 = forced expiratory volume in 1 second, CF = cystic fibrosis.
Reference
-
1. Ratjen F, Döring G. Cystic fibrosis. Lancet. 2003; 361:681–689.2. Kliegman RM, Stanton BF, St. Geme JW 3rd, Schor NF. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier Saunders;2016.3. Ong T, Ramsey BW. Update in cystic fibrosis 2014. Am J Respir Crit Care Med. 2015; 192:669–675.4. Farrell PM, White TB, Ren CL, Hempstead SE, Accurso F, Derichs N, Howenstine M, McColley SA, Rock M, Rosenfeld M, et al. Diagnosis of cystic fibrosis: consensus guidelines from the cystic fibrosis foundation. J Pediatr. 2017; 181S:S4–S15.5. Thabut G, Christie JD, Mal H, Fournier M, Brugière O, Leseche G, Castier Y, Rizopoulos D. Survival benefit of lung transplant for cystic fibrosis since lung allocation score implementation. Am J Respir Crit Care Med. 2013; 187:1335–1340.6. Vandemheen KL, O'Connor A, Bell SC, Freitag A, Bye P, Jeanneret A, Berthiaume Y, Brown N, Wilcox P, Ryan G, et al. Randomized trial of a decision aid for patients with cystic fibrosis considering lung transplantation. Am J Respir Crit Care Med. 2009; 180:761–768.7. Liou TG, Adler FR, Cox DR, Cahill BC. Lung transplantation and survival in children with cystic fibrosis. N Engl J Med. 2007; 357:2143–2152.8. Crawford TC, Dickinson K, Magruder JT, Grimm JC, Bush EL, Kim BS, Merlo CA. Cystic fibrosis and pediatric lung transplantation: improved survival in the lung allocation score era. Am J Respir Crit Care Med. 2017; 195:A4849.9. Yamashiro Y, Shimizu T, Oguchi S, Shioya T, Nagata S, Ohtsuka Y. The estimated incidence of cystic fibrosis in Japan. J Pediatr Gastroenterol Nutr. 1997; 24:544–547.10. Jung H, Ki CS, Koh WJ, Ahn KM, Lee SI, Kim JH, Ko JS, Seo JK, Cha SI, Lee ES, et al. Heterogeneous spectrum of CFTR gene mutations in Korean patients with cystic fibrosis. Korean J Lab Med. 2011; 31:219–224.11. Rosenblatt RL. Lung transplantation in cystic fibrosis. Respir Care. 2009; 54:777–786.12. Kirkby S, Hayes D Jr. Pediatric lung transplantation: indications and outcomes. J Thorac Dis. 2014; 6:1024–1031.13.13. Goldfarb SB, Levvey BJ, Edwards LB, Dipchand AI, Kucheryavaya AY, Lund LH, Meiser B, Rossano JW, Yusen RD, Stehlik J, et al. The registry of the international society for heart and lung transplantation: nineteenth pediatric lung and heart-lung transplantation report-2016; focus theme: primary diagnostic indications for transplant. J Heart Lung Transplant. 2016; 35:1196–1205.14. Sato M, Okada Y, Oto T, Minami M, Shiraishi T, Nagayasu T, Yoshino I, Chida M, Okumura M, Date H, et al. Registry of the Japanese Society of Lung and Heart-Lung Transplantation: official Japanese lung transplantation report, 2014. Gen Thorac Cardiovasc Surg. 2014; 62:594–601.15. Adler FR, Aurora P, Barker DH, Barr ML, Blackwell LS, Bosma OH, Brown S, Cox DR, Jensen JL, Kurland G, et al. Lung transplantation for cystic fibrosis. Proc Am Thorac Soc. 2009; 6:619–3316.16. Jhang WK, Park SJ, Lee E, Yang SI, Hong SJ, Seo JH, Kim HY, Park JJ, Yun TJ, Kim HR, et al. The first successful heart-lung transplant in a Korean child with humidifier disinfectant-associated interstitial lung disease. J Korean Med Sci. 2016; 31:817–821.17. Folescu TW, da Costa CH, Cohen RW, da Conceição Neto OC, Albano RM, Marques EA. Burkholderia cepacia complex: clinical course in cystic fibrosis patients. BMC Pulm Med. 2015; 15:158.18. Hollander FM, van Pierre DD, de Roos NM, van de Graaf EA, Iestra JA. Effects of nutritional status and dietetic interventions on survival in Cystic Fibrosis patients before and after lung transplantation. J Cyst Fibros. 2014; 13:212–218.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anesthetic experience in patient for single lung transplantation with previous contralateral pneumonectomy: A case report
- Cystic Fibrosis: Case Report
- Cystic fibrosis lung disease: Current perspectives
- Combined Bilateral Lung Transplantation and Off-Pump Coronary Artery Bypass
- Radiologic Findings of Cystic Fibrosis in a Korean Child at Follow Up Study: Case Report
