Ann Pediatr Endocrinol Metab.
2017 Sep;22(3):208-212. 10.6065/apem.2017.22.3.208.
Delayed diagnosis of pituitary stalk interruption syndrome with severe recurrent hyponatremia caused by adrenal insufficiency
- Affiliations
-
- 1Department of Pediatrics, Yeungnam University College of Medicine, Daegu, Korea.
- 2Department of Pediatric Endocrinology, Kyungpook National University Children’s Hospital, Daegu, Korea. cwko@knu.ac.kr
- KMID: 2396142
- DOI: http://doi.org/10.6065/apem.2017.22.3.208
Abstract
- Pituitary stalk interruption syndrome (PSIS) involves the occurrence of a thin or absent pituitary stalk, hypoplasia of the adenohypophysis, and ectopic neurohypophysis. Diagnosis is confirmed using magnetic resonance imaging. Patients with PSIS have a variable degree of pituitary hormone deficiency and a wide spectrum of clinical manifestations. The clinical course of the disease in our patient is similar to that of a syndrome of inappropriate antidiuretic hormone secretion. This is thought to be caused by failure in the suppression of vasopressin secretion due to hypocortisolism. To the best of our knowledge, there is no case report of a patient with PSIS presenting with hyponatremia as the first symptom in Korean children. Herein, we report a patient with PSIS presenting severe recurrent hyponatremia as the first symptom, during adolescence and explain the pathophysiology of hyponatremia with secondary adrenal insufficiency.
Keyword
MeSH Terms
Figure
-

Fig. 1. The patient's height from 6 to 13 years of age was based on school physical records and was not measured in the last 8 years. The growth curve showed markedly short stature and growth rates less than 5 cm/yr during childhood.

Fig. 2. The left-hand anteroposterior view represents between 14 and 15 years of bone age using the standards of the Greulich-Pyle method, which is delayed compared to chronological age of 24 year-old.
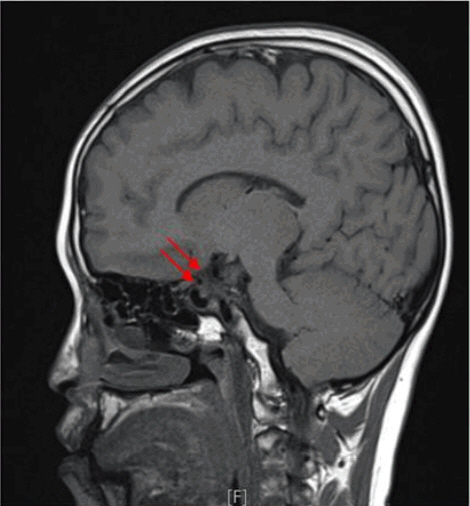
Fig. 3. The arrows indicate absent pituitary stalk, hypoplasia of the adenohypophysis, and absent posterior pituitary gland on sella magnetic resonance imaging.
Reference
-
References
1. Fujisawa I, Kikuchi K, Nishimura K, Togashi K, Itoh K, Noma S, et al. et al. Transection of the pituitary stalk: development of an ectopic posterior lobe assessed with MR imaging. Radiology. 1987; 165:487–9.
Article2. Arrigo T, Wasniewska M, De Luca F, Valenzise M, Lombardo F, Vivenza D, et al. Congenital adenohypophysis aplasia: clinical features and analysis of the transcriptional factors for embryonic pituitary development. J Endocrinol Invest. 2006; 29:208–13.
Article3. Olszewska M, Kiełbasa G, Wójcik M, Zygmunt-Górska A, Starzyk JB. A case report of severe panhypopituitarism in a newborn delivered by a women with Turner syndrome. Neuro Endocrinol Lett. 2015; 36:734–6.4. Marmouch H, Graja S, Arfa S, Boubaker F, Khochtali I. Late-onset pituitary stalk interruption syndrome (PSIS). Pan Afr Med J. 2016; 23:108.5. Kim SY. Diagnosis and treatment of hypopituitarism. Endocrinol Metab (Seoul). 2015; 30:443–55.
Article6. Diederich S, Franzen NF, Bähr V, Oelkers W. Severe hyponatremia due to hypopituitarism with adrenal insufficiency: report on 28 cases. Eur J Endocrinol. 2003; 148:609–17.
Article7. Bartter FC, Schwartz WB. The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1967; 42:790–806.
Article8. Oelkers W. Hyponatremia and inappropriate secretion of vasopressin (antidiuretic hormone) in patients with hypopituitarism. N Engl J Med. 1989; 321:492–6.
Article9. Erkut ZA, Pool C, Swaab DF. Glucocorticoids suppress corticotropin-releasing hormone and vasopressin expression in human hypothalamic neurons. J Clin Endocrinol Metab. 1998; 83:2066–73.
Article10. Raff H. Glucocorticoid inhibition of neurohypophysial vasopressin secretion. Am J Physiol. 1987; 252(4 Pt 2):R635–44.
Article11. Puar TH, Stikkelbroeck NM, Smans LC, Zelissen PM, Hermus AR. Adrenal crisis: still a deadly event in the 21st century. Am J Med. 2016; 129:339. e1-9.
Article12. Cuesta M, Garrahy A, Slattery D, Gupta S, Hannon AM, Forde H, et al. The contribution of undiagnosed adrenal insufficiency to euvolaemic hyponatraemia: results of a large prospective single-centre study. Clin Endocrinol (Oxf). 2016; 85:836–44.
Article13. Verbalis JG, Goldsmith SR, Greenberg A, Korzelius C, Schrier RW, Sterns RH, et al. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013; 126(10 Suppl 1):S1–42.
Article14. Deodati A, Cianfarani S. Impact of growth hormone therapy on adult height of children with idiopathic short stature: systematic review. BMJ. 2011; 342:c7157.
Article15. Damiani D, Damiani D. Pharmacological management of children with short stature: the role of aromatase inhibitors. J Pediatr (Rio J). 2007; 83(5 Suppl):S172–7.
Article16. Kwon JH, Lee HA, Kim YJ, Lee H, Park EA, Cho SJ, et al. Effects of adrenal androgen levels on bone age advancement in prepubertal children: using the Ewha Birth and Growth Cohort Study. J Korean Med Sci. 2017; 32:968–73.
Article17. John S, PaE I, Felner . Kliegman RM, Stanton B, Geme J, Schor N, editors. Nelson textbook of pediatrics. 20th ed. Philadelphia: Elsevier Saunders;2016. p. 2643–3.18. Mauras N, Attie KM, Reiter EO, Saenger P, Baptista J. High dose recombinant human growth hormone (GH) treatment of GH-deficient patients in puberty increases near-final height: a randomized, multicenter trial. Genentech, Inc., Cooperative Study Group. J Clin Endocrinol Metab. 2000; 85:3653–60.19. Reynaud R, Albarel F, Saveanu A, Kaffel N, Castinetti F, Lecomte P, et al. Pituitary stalk interruption syndrome in 83 patients: novel HESX1 mutation and severe hormonal prognosis in malformative forms. Eur J Endocrinol. 2011; 164:457–65.
Article20. Wang CZ, Guo LL, Han BY, Su X, Guo QH, Mu YM. Pituitary stalk interruption syndrome: from clinical findings to pathogenesis. J Neuroendocrinol. 2017; 29:https://doi.org/10.1111/jne.12451.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic hyponatremia of Sheehan's syndrome
- A Case of Giant Cell Granulomatous Hypophysitis with Recurrent Hypoosmolar Hyponatremia
- A Case of Pituitary Stalk Interruption Syndrome in Early Childhood Presenting with Congenital Hypothyroidism
- A Case of Severe Hyponatremia Associated with Hypopituitarism due to Hemorrhagic Fever with Renal Syndrome
- Pituitary Stalk Transection Syndrome
