A Prospective Study with Cage-Only or Cage-with-Plate Fixation in Anterior Cervical Discectomy and Interbody Fusion of One and Two Levels
- Affiliations
-
- 1Department of Neurosurgery, Inha University School of Medicine, Incheon, Korea. nsyoon@gmail.com
- 2Guri Cham Teun Teun Hospital, Guri, Korea.
- KMID: 2395789
- DOI: http://doi.org/10.3340/jkns.2017.0211
Abstract
OBJECTIVE
The authors prospectively analyzed the effect of one-level or two-level anterior cervical discectomy and fusion (ACDF), comparing stand-alone cages and cage-with-plate fixation constructs with respect to clinical outcomes and radiologic changes.
METHODS
A total of 84 patients who underwent one-level (n=52) or two-level ACDF (n=32) for cervical disc disease and who completed 2 years of follow-up were included in this study. The patients were divided by cervical level and grouped into ACDF-Cage-only and ACDF-Cage-with-plate groups. The following parameters were assessed using radiographs: subsidence, C2-C7 lordosis angle, fusion segment angle, adjacent disc space narrowing, and fusion status. Clinical outcomes were assessed using the neck disability index (NDI) and visual analog scale scores for arm pain.
RESULTS
In the comparison of one-level ACDF-cage-only and ACDF-cage-with-plate groups, the NDI score was better in the cage-only group at the 3-, 12-, and 24-month follow-ups: however, no significant difference in clinical outcomes was observed. In the comparison of two-level ACDF-cage-only and ACDF-cage-with-plate groups, no difference in any clinical outcome was observed between the two groups. At the 24-month follow-up, subsidence was observed in 45.8% of patients in the one-level cage-only group and 32.1% of patients in the one-level cage-with-plate fixation group. There was no statistically significant difference in the incidence rate between the two groups (p=0.312). Subsidence in the two-level cage-only group (66.6%) was significantly more frequent than in the two-level cage-with-plate fixation group (30%; p=0.049). The fusion rate for patients in the one-level cage-only group was not significantly different from that in the one-level cage-with-plate fixation group (cage-only, 87.5%; cage-with-plate fixation, 92.9%; p=0.425); fusion rate in the two-level patients were also similar between groups (cage-only, 83.3%; cage-with-plate fixation, 95%; p=0.31).
CONCLUSION
Our clinical results showed that for single-level cases, plate fixation had no additional benefit versus cage-only; for two-level ACDF cases, the fusion rate and clinical outcomes were similar, although the cage-with-plate fixation group had a lower incidence of cage subsidence than did the cage-only group. We conclude that physicians should be aware of this possible disadvantage associated with using cervical plates in one-level ACDF. However, in two-level ACDF, subsidence is more likely to occur without plate fixation, and thus the addition of plate fixation should be considered.
Keyword
MeSH Terms
Figure
-

Fig. 1 A: The adjacent disc mid-height (mm) was measured, and adjacent disc degeneration was compared. B: Subsidence was defined as the condition when the distance (mm) between the midpoint of the upper vertebra of the fusion segment, and the midpoint of the inferior endplate of the lower vertebra showed a difference of more than 2 mm between the pre-operative and 24-month X-rays. C: Fusion segment angle: Cobb’s angle (°) between the superior endplate of the upper vertebra of the fusion segment and the inferior endplate of the lower vertebra was measured from the lateral plain radiograph. D: To assess global cervical lordosis, Cobb’s angle (°) between the posterior margin of the C2 and C7 vertebral bodies was measured.
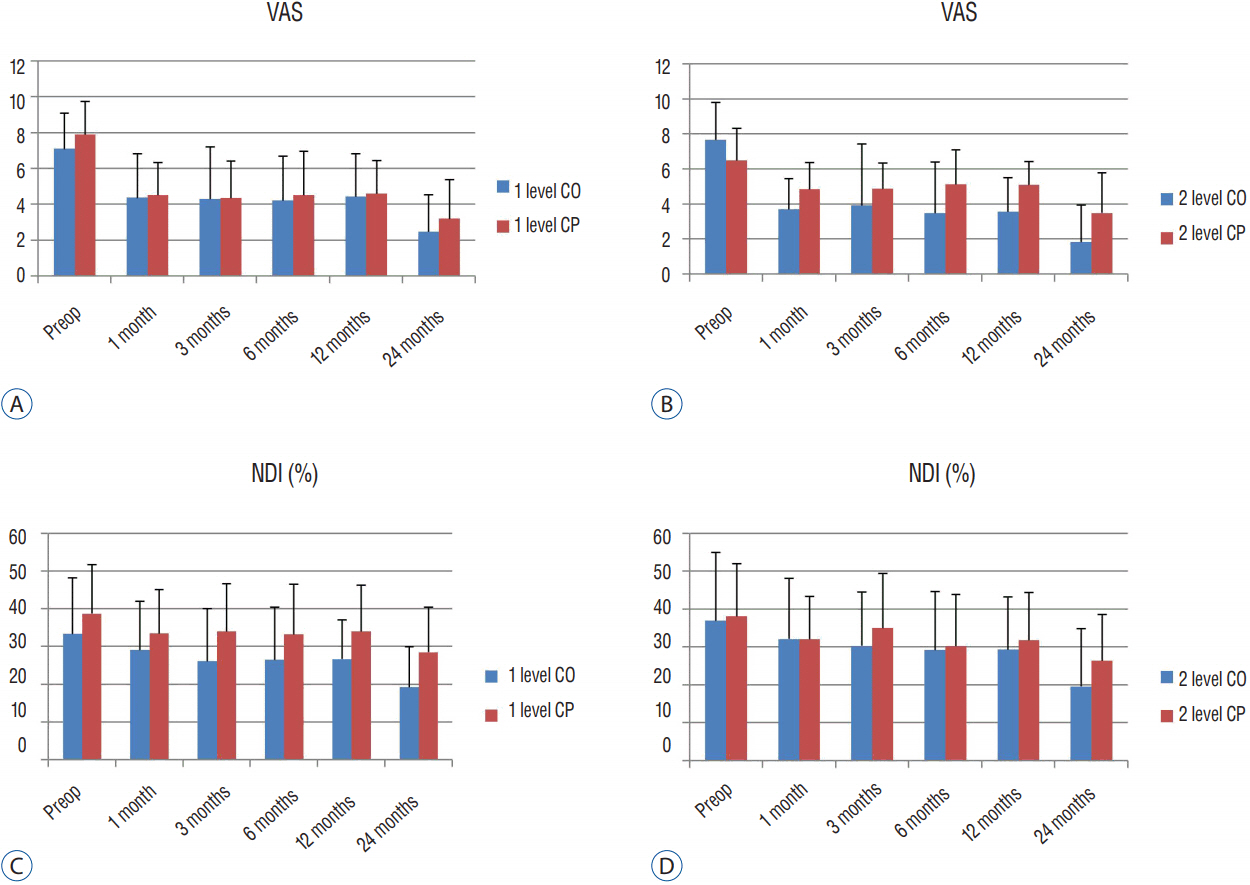
Fig. 2 A and B: Comparison of visual analog scale (VAS) score (Arm) between one-level cage-only (CO) vs. cage-with-plate (CP) (A) and two-level CO vs. CP fixation (B). C and D: Comparison of neck disability index (NDI) scores between one-level CO vs. CP (C) and two-level CO vs. CP fixation (D).

Fig. 3 A and B: Comparison of C2–7 angle (°) between one-level cage-only (CO) vs. cage-with-plate (CP) (A) and two-level CO vs. CP fixation (B). C and D: Comparison of the fusion segmental angle (°) between one-level CO vs. CP (C) and two-level CO vs. CP fixation (D). E and F: Comparison of the adjacent disc height (lower, mm) between one-level CO vs. CP (E) and two-level CO vs. CP fixation (F). G and H: Comparison of the adjacent disc height (upper, mm) between one-level CO vs. CP (G) and two-level CO vs. CP fixation (H).
Reference
-
References
1. Ahn SS, Paik HK, Chin DK, Kim SH, Kim DW, Ku MG. The fate of adjacent segments after anterior cervical discectomy and fusion: the influence of an anterior plate system. World Neurosurg. 89:42–50. 2016.
Article2. Cho DY, Lee WY, Sheu PC. Treatment of multilevel cervical fusion with cages. Surg Neurol. 62:378–385. discussion 385–6. 2004.
Article3. Choi MK, Kim SB, Park CK, Kim SM. Comparison of the clinical and radiologic outcomes obtained with single- versus two-level anterior cervical decompression and fusion using stand-alone PEEK cages filled with allograft. Acta Neurochir (Wien). 158:481–487. 2016.
Article4. Demircan MN, Kutlay AM, Colak A, Kaya S, Tekin T, Kibici K, et al. Multilevel cervical fusion without plates, screws or autogenous iliac crest bone graft. J Clin Neurosci. 14:723–728. 2007.
Article5. El-Tantawy A. Is it possible to eliminate the plate-related problems and still achieve satisfactory outcome after multilevel anterior cervical discectomy? Eur J Orthop Surg Traumatol. 25(Suppl 1):135–145. 2015.
Article6. Fountas KN, Kapsalaki EZ, Nikolakakos LG, Smisson HF, Johnston KW, Grigorian AA, et al. Anterior cervical discectomy and fusion associated complications. Spine (Phila Pa 1976). 32:2310–2317. 2007.
Article7. Fraser JF, Härtl R. Anterior approaches to fusion of the cervical spine: a metaanalysis of fusion rates. J Neurosurg Spine. 6:298–303. 2007.
Article8. Han SY, Kim HW, Lee CY, Kim HR, Park DH. Stand-alone cages for anterior cervical fusion: are there no problems? Korean J Spine. 13:13–19. 2016.
Article9. Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the consequences of spinal fusion? Spine J. 4(6 Suppl):190S–194S. 2004.
Article10. Jacobs W, Willems PC, Kruyt M, van Limbeek J, Anderson PG, Pavlov P, et al. Systematic review of anterior interbody fusion techniques for single- and double-level cervical degenerative disc disease. Spine (Phila Pa 1976). 36:E950–E960. 2011.
Article11. Ji GY, Oh CH, Shin DA, Ha Y, Kim KN, Yoon DH, et al. Stand-alone cervical cages versus anterior cervical plates in 2-level cervical anterior interbody fusion patients: analysis of adjacent segment degeneration. J Spinal Disord Tech. 28:E433–E438. 2015.12. Joo YH, Lee JW, Kwon KY, Rhee JJ, Lee HK. Comparison of fusion with cage alone and plate instrumentation in two-level cervical degenerative disease. J Korean Neurosurg Soc. 48:342–346. 2010.
Article13. Kast E, Derakhshani S, Bothmann M, Oberle J. Subsidence after anterior cervical inter-body fusion. A randomized prospective clinical trial. Neurosurg Rev. 32:207–214. discussion 214. 2009.
Article14. Kim MK, Kim SM, Jeon KM, Kim TS. Radiographic comparison of four anterior fusion methods in two level cervical disc diseases: autograft plate fixation versus cage plate fixation versus stand-alone cage fusion versus corpectomy and plate fixation. J Korean Neurosurg Soc. 51:135–40. 2012.
Article15. Lee CH, Hyun SJ, Kim MJ, Yeom JS, Kim WH, Kim KJ, et al. Comparative analysis of 3 different construct systems for single-level anterior cervical discectomy and fusion: stand-alone cage, iliac graft plus plate augmentation, and cage plus plating. J Spinal Disord Tech. 26:112–118. 2013.
Article16. Lee YS, Kim YB, Park SW. Risk factors for postoperative subsidence of single-level anterior cervical discectomy and fusion: the significance of the preoperative cervical alignment. Spine (Phila Pa 1976). 39:1280–1287. 2014.
Article17. Li J, Li Y, Kong F, Zhang D, Zhang Y, Shen Y. Adjacent segment degeneration after single –level anterior cervical decompression and fusion: disc space distraction and its impact on clinical outcomes. J Clin Neurosci. 22:566–569. 2015.
Article18. Litrico S, Lonjon N, Riouallon G, Cogniet A, Launay O, Beaurain J, et al. Adjacent segment disease after anterior cervical interbody fusion: a multicenter retrospective study of 288 patients with long-term follow-up. Orthop Traumatol Surg Res. 100(6 Suppl):S305–S309. 2014.
Article19. Nambiar M, Phan K, Cunningham JE, Yang Y, Turner PL, Mobbs R. Locking stand-alone cages versus anterior plate constructs in single-level fusion for degenerative cervical disease: a systematic review and meta-analysis. Eur Spine J. 26:2258–2266. 2017.
Article20. Oh JK, Kim TY, Lee HS, You NK, Choi GH, Yi S, et al. Stand-alone cervical cages versus anterior cervical plate in 2-level cervical anterior interbody fusion patients: clinical outcomes and radiologic changes. J Spinal Disord Tech. 26:415–420. 2013.
Article21. Oh K, Lee CK, You NK, Kim SH, Cho KH. Radiologic changes of anterior cervical discectomy and fusion using allograft and plate augmentation: comparison of using fixed and variable type screw. Korean J Spine. 10:160–164. 2013.
Article22. Park SB, Chung CK, Lee SH, Yang HJ, Son YJ, Chung YS. The impact of menopause on bone fusion after the single-level anterior cervical discectomy and fusion. J Korean Neurosurg Soc. 54:496–500. 2013.
Article23. Pereira EA, Chari A, Hempenstall J, Leach JC, Chandran H, Cadoux-Hudson TA. Anterior cervical discectomy plus intervertebral polyetheretherketone cage fusion over three and four levels without plating is safe and effective long-term. J Clin Neurosci. 20:1250–1255. 2013.
Article24. Resnick DK, Trost GR. Use of ventral plates for cervical arthrodesis. Neurosurgery. 60(1 Suppl 1):S112–S117. 2007.
Article25. Shiban E, Gapon K, Wostrack M, Meyer B, Lehmberg J. Clinical and radiologic outcome after anterior cervical discectomy and fusion with stand-alone empty polyetheretherketone (PEEK) cages. Acta Neurochir (Wien). 158:349–355. 2016.
Article26. Singh P, Kumar A, Shekhawat V. Comparative analysis of interbody cages versus tricortical graft with anterior plate fixation for anterior cervical discectomy and fusion in degenerative cervical disc disease. J Clin Diagn Res. 10:RC05–RC08. 2016.
Article27. Song KJ, Choi BW, Kim JK. Adjacent segment pathology following anterior decompression and fusion using cage and plate for the treatment of degenerative cervical spinal diseases. Asian Spine J. 8:720–728. 2014.
Article28. Song KJ, Taghavi CE, Lee KB, Song JK, Eun JP. The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Spine (Phila Pa 1976). 34:2886–2892. 2009.
Article29. Wang JC, McDonough PW, Endow KK, Delamarter RB. Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion. Spine (Phila Pa 1976). 25:41–45. 2000.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anterior Cervical Bisegmental Interbody Fusion with Titanium Cage(RABEA) in Degenerative Cervical Disease: Comparative Analysis with Monosegmental Interbody Fusion
- Anterior Cervical Interbody Fusion Using a Plate Cage System in Degenerative Cervical Disease
- Efficiency of Anterior Interbody Fusion using Cage and Plate in the Distractive Flexion Injury of Cervical Spine : Cage vs Tricortical Autoiliac Bone
- The Advantages of Rectangular Titanium Cage(RABEA) Fusion after Anterior Cervical Discectomy: Comparative Study of Fibula Allograft
- Clinical Results of Anterior Cervical Discectomy and Fusion with Prefilled Cage in Patient with Traumatic Cervical Injury
