J Korean Ophthalmol Soc.
2017 Oct;58(10):1194-1198. 10.3341/jkos.2017.58.10.1194.
Cryotherapy on Refractory Fungal Corneal Ulcer: A Case Report
- Affiliations
-
- 1Department of Ophthalmology, Chosun University College of Medicine, Gwangju, Korea. ophkoh@hanmail.net
- KMID: 2393173
- DOI: http://doi.org/10.3341/jkos.2017.58.10.1194
Abstract
- PURPOSE
We report a case of cryotherapy for fungal corneal ulcers that did not respond to antifungal agents.
CASE SUMMARY
A 58-year-old man was transferred to our hospital with a left eye corneal ulcer due to pain and visual impairment in his left eye for two weeks, and he was suspected to have a history of fungal infection. At the time of admission, corneal opacity and progressive ulcerative lesions were observed at 5 o'clock in the left eye and visual acuity was 0.025, uncorrected. The corneal ulcer marginal resection, bacterial culture, and potassium hydroxide preparation (KOH) test were performed on lesion sites. Cultures of Candida albicans were reported to grow, topical antibiotics (Fortified tobramycin, Fortified cefazolin, moxifloxacin), and anti-fungal agents (fortified amphotericin B, 0.5%, Natamycin) were administered, but no improvement was observed for 2 weeks. On the 14th day after admission, Cryotherapy was performed. After surgery, eye drops were equally applied, and there was no other discomfort other than pain for 3 days after the operation. He discharged 10 days after surgery, the corneal lesion was healed and the visual acuity was improved to 0.32, uncorrected.
CONCLUSIONS
We report a case of cryotherapy for fungal corneal ulcers that did not react with topical antifungal drugs and improved visual acuity and symptom improvement.
MeSH Terms
-
Amphotericin B
Anti-Bacterial Agents
Antifungal Agents
Candida albicans
Cefazolin
Corneal Opacity
Corneal Ulcer*
Cryotherapy*
Humans
Middle Aged
Ophthalmic Solutions
Potassium
Tobramycin
Ulcer
Vision Disorders
Visual Acuity
Amphotericin B
Anti-Bacterial Agents
Antifungal Agents
Cefazolin
Ophthalmic Solutions
Potassium
Tobramycin
Figure
-

Figure 1 Anterior segment photo of the patient who did not show improvement in medical treatment for 2 weeks. 2 weeks after medical treatment, (A) corneal opacity and progressive infiltrative lesion still observed at 5 o'clock in the left eye. (B) Cornea epithelial defect with ulcerative lesion observed in the cornea at 5 o'clock after stining.

Figure 2 Photo of cryotherapy. Cryotherapy was performed on 5 o'clock of progressive ulcerative and infiltrative lesion refractory to previous medical treatment.
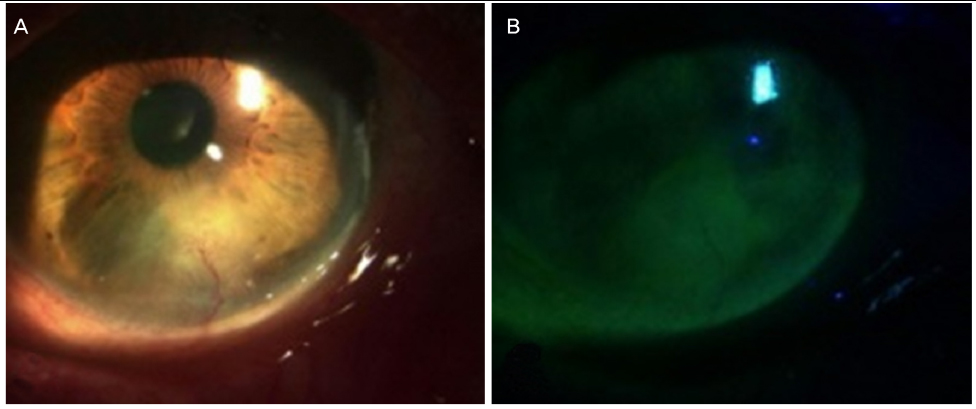
Figure 3 2 months after cryotherapy. (A) Corneal neovascularization and corneal opacity remain, since 5 o'clock cornea lesion completely healed. (B) Corneal epithelium defect was fully recovered.
Reference
-
1. Hahn YH, Lee DJ, Kim MS, et al. Epidemiology of Fungal Keratitis in Korea: a multi-center study. J Korean Ophthalmol Soc. 2000; 41:1499–1508.2. O'Day DM. Selection of appropriate antifungal therapy. Cornea. 1987; 6:238–245.3. Thomas PA. Fungal infections of the cornea. Eye (Lond). 2003; 17:852–862.4. Rosa RH Jr, Miller D, Alfonso EC. The changing spectrum of fungal keratitis in south Florida. Ophthalmology. 1994; 101:1005–1013.5. Lalitha P, Prajna NV, Kabra A, et al. Risk factors for treatment outcome in fungal keratitis. Ophthalmology. 2006; 113:526–530.6. Xie L, Zhai H, Shi W. Penetrating keratoplasty for corneal perforations in fungal keratitis. Cornea. 2007; 26:158–162.7. Chen Y, Yang W, Gao M, et al. Experimental study on cryotherapy for fungal corneal ulcer. BMC Ophthalmol. 2015; 15:29.8. Arora S, Tyragi SC. Fungal flora of conjunctival sac in health and disease. Indian J Ophthalmol. 1976; 24:15–18.9. Ando N, Takatori K. Fungal flora of the conjunctival sac. Am J Ophthalmol. 1982; 94:67–74.10. Wilson LA, Ahearn DG, Jones DB, Sexton RR. Fungi from the normal outer eye. Am J Ophthalmol. 1969; 67:52–56.11. Alfonso EC, Rosa RH, Miller D. Fungal keratitis. In : Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 3rd ed. Vol. 1. New York: Mosby Elsevier Inc;2011. chap. 82.12. Ghannoum MA, Rice LB. Antifungal agents: mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Clin Microbiol Rev. 1999; 12:501–517.13. Lee KH, Ghae HJ, Yoon KC. Analysis of risk factors for treatment failure in fungal keratitis. J Korean Ophthalmol Soc. 2008; 49:737–742.14. Mannis MJ. Conjunctival flaps. Int Ophthalmol Clin. 1988; 28:165–168.15. Sullivan JH. Cryosurgery in ophthalmic practice. Ophthalmic Surg. 1979; 10:37–41.16. Wilkes TD, Fraunfelder FT. Principles of cryosurgery. Ophthalmic Surg. 1979; 10:21–30.17. Ebrahimi KB, Green WR, Grebe R, Jun AS. Acanthamoeba sclerokeratitis. Graefes Arch Clin Exp Ophthalmol. 2009; 247:283–286.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Human Amniotic Membrane Transplantation for Treatment of Fungal Ulcer
- A Case of Fungal Keratitis as a Complication of Orthokeratology Contact Lens
- A Case of Fusarium solani Keratitis mixed by Acremonium falciforme
- Multilayer Collagen Sheet Graft for Corneal Perforation with a Corneal Ulcer
- The Amniotic Membrane Transplantation in Corneal Perforation due to Mooren's Ulcer
