Liver Abscess Formation after Radiofrequency Ablation of Hepatocellular Carcinoma
- Affiliations
-
- 1Department of Radiology, Seoul Veterans Hospital, Seoul, Korea. yunkucho2004@yahoo.co.kr
- KMID: 2392119
- DOI: http://doi.org/10.3348/jksr.2017.77.4.229
Abstract
- PURPOSE
To determine prognostic factors for the development of liver abscess formation in patients with hepatocellular carcinoma (HCC) treated with radiofrequency ablation (RFA) focusing on the history of multiple prior sessions of transarterial chemoembolization (TACE).
MATERIALS AND METHODS
Patients were included if RFA was performed from January 2005 to July 2016 for a single HCC nodule smaller than or equal to 5 cm or up to three nodules with each nodule smaller than or equal to 3 cm. Univariate and multivariate logistic regression analyses were conducted and propensity score matching was performed between those without multiple prior sessions of TACE before ablation (Group 1) and those with such a history (Group 2).
RESULTS
Overall, 694 patients were included in this study. Liver abscesses were developed in four patients, all in Group 2. After performing 2:1 propensity score matching, 149 and 81 patients were selected for Group 1 and 2, respectively. Among these matched patients, rates of liver abscess development were 0% and 5.1% in Group 1 and 2, respectively. The difference in rate of liver abscess development between the two groups was statistically significant (p = 0.014).
CONCLUSION
A history of multiple prior TACE sessions was a potent predictor for liver abscess formation in patients with HCC after performing RFA.
MeSH Terms
Figure
-
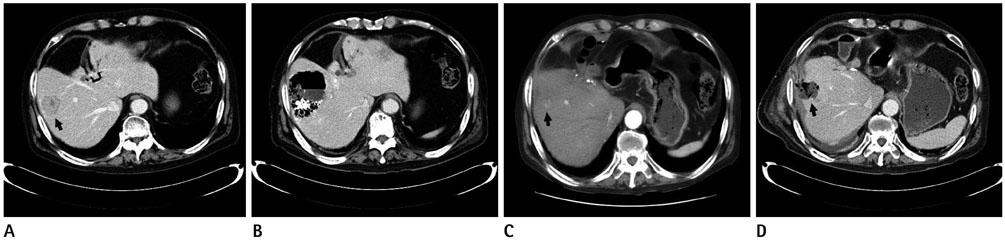
Fig. 1 A 72-year-old male patient with hepatocellular carcinoma. A. Pre-treatment post-contrast portal phase CT image showing a 2.5 cm sized hepatic nodule (arrow) diagnosed histopathologically as hepatocellular carcinoma. B. Post-contrast CT scan performed one month after two repetitive transarterial chemoembolization showing a large liver abscess at the same site which was resolved with conservative management. C. Post-contrast CT scan performed nine months after the last transarterial chemoembolization demonstrating a local tumor progression at the previous ablation site (arrow). Radiofrequency ablation was again performed to treat the local tumor progression. D. Post-contrast CT scan performed one week after performing radiofrequency ablation showing a liver abscess (arrow) at the ablation site, extending into adjacent abdominal wall. The abscess was resolved with conservative management.
Reference
-
1. El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999; 340:745–750.2. Shiina S, Tateishi R, Arano T, Uchino K, Enooku K, Nakagawa H, et al. Radiofrequency ablation for hepatocellular carcinoma: 10-year outcome and prognostic factors. Am J Gastroenterol. 2012; 107:569–577. quiz 578.3. Peng ZW, Lin XJ, Zhang YJ, Liang HH, Guo RP, Shi M, et al. Radiofrequency ablation versus hepatic resection for the treatment of hepatocellular carcinomas 2 cm or smaller: a retrospective comparative study. Radiology. 2012; 262:1022–1033.4. Nakazawa T, Kokubu S, Shibuya A, Ono K, Watanabe M, Hidaka H, et al. Radiofrequency ablation of hepatocellular carcinoma: correlation between local tumor progression after ablation and ablative margin. AJR Am J Roentgenol. 2007; 188:480–488.5. Lee DH, Lee JM, Lee JY, Kim SH, Yoon JH, Kim YJ, et al. Radiofrequency ablation of hepatocellular carcinoma as first-line treatment: long-term results and prognostic factors in 162 patients with cirrhosis. Radiology. 2014; 270:900–909.6. Kei SK, Rhim H, Choi D, Lee WJ, Lim HK, Kim YS. Local tumor progression after radiofrequency ablation of liver tumors: analysis of morphologic pattern and site of recurrence. AJR Am J Roentgenol. 2008; 190:1544–1551.7. de Baère T, Risse O, Kuoch V, Dromain C, Sengel C, Smayra T, et al. Adverse events during radiofrequency treatment of 582 hepatic tumors. AJR Am J Roentgenol. 2003; 181:695–700.8. Choi D, Lim HK, Kim MJ, Kim SJ, Kim SH, Lee WJ, et al. Liver abscess after percutaneous radiofrequency ablation for hepatocellular carcinomas: frequency and risk factors. AJR Am J Roentgenol. 2005; 184:1860–1867.9. Mulier S, Mulier P, Ni Y, Miao Y, Dupas B, Marchal G, et al. Complications of radiofrequency coagulation of liver tumours. Br J Surg. 2002; 89:1206–1222.10. Livraghi T, Solbiati L, Meloni MF, Gazelle GS, Halpern EF, Goldberg SN. Treatment of focal liver tumors with percutaneous radio-frequency ablation: complications encountered in a multicenter study. Radiology. 2003; 226:441–451.11. Morimoto M, Numata K, Kondo M, Moriya S, Morita S, Maeda S, et al. Radiofrequency ablation combined with transarterial chemoembolization for subcapsular hepatocellular carcinoma: a prospective cohort study. Eur J Radiol. 2013; 82:497–503.12. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012; 379:1245–1255.13. Kim JH, Won HJ, Shin YM, Kim SH, Yoon HK, Sung KB, et al. Medium-sized (3.1-5.0 cm) hepatocellular carcinoma: transarterial chemoembolization plus radiofrequency ablation versus radiofrequency ablation alone. Ann Surg Oncol. 2011; 18:1624–1629.14. Bruix J, Sherman M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005; 42:1208–1236.15. Lang EV, Chen F, Fick LJ, Berbaum KS. Determinants of intravenous conscious sedation for arteriography. J Vasc Interv Radiol. 1998; 9:407–412.16. Ahmed M, Solbiati L, Brace CL, Breen DJ, Callstrom MR, Charboneau JW, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria--a 10-year update. J Vasc Interv Radiol. 2014; 25:1691–1705.e4.17. Mori K, Fukuda K, Asaoka H, Ueda T, Kunimatsu A, Okamoto Y, et al. Radiofrequency ablation of the liver: determination of ablative margin at MR imaging with impaired clearance of ferucarbotran--feasibility study. Radiology. 2009; 251:557–565.18. Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Major complications after radio-frequency thermal ablation of hepatic tumors: spectrum of imaging findings. Radiographics. 2003; 23:123–134. discussion 134-136.19. Song SY, Chung JW, Han JK, Lim HG, Koh YH, Park JH, et al. Liver abscess after transcatheter oily chemoembolization for hepatic tumors: incidence, predisposing factors, and clinical outcome. J Vasc Interv Radiol. 2001; 12:313–320.20. Kim W, Clark TW, Baum RA, Soulen MC. Risk factors for liver abscess formation after hepatic chemoembolization. J Vasc Interv Radiol. 2001; 12:965–968.21. Kim MH, Choi MS, Choi YS, Kim DY, Lee JM, Paik SW, et al. Clinical features of liver abscess developed after radiofrequency ablation and transarterial chemoembolization for hepatocellular carcinoma. Korean J Hepatol. 2006; 12:55–64.22. Kobayashi S, Nakanuma Y, Terada T, Matsui O. Postmortem survey of bile duct necrosis and biloma in hepatocellular carcinoma after transcatheter arterial chemoembolization therapy: relevance to microvascular damages of peribiliary capillary plexus. Am J Gastroenterol. 1993; 88:1410–1415.23. de Baère T, Roche A, Amenabar JM, Lagrange C, Ducreux M, Rougier P, et al. Liver abscess formation after local treatment of liver tumors. Hepatology. 1996; 23:1436–1440.24. Chen C, Chen PJ, Yang PM, Huang GT, Lai MY, Tsang YM, et al. Clinical and microbiological features of liver abscess after transarterial embolization for hepatocellular carcinoma. Am J Gastroenterol. 1997; 92:2257–2259.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Completely Ablated Hepatocellular Carcinoma by Percutaneous Radiofrequency Thermal Ablation
- Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
- A Delayed Hepatico-colonic Fistula after Radiofrequency Ablation in Hepatocellular Carcinoma
- Biliary-duodenal Fistula Following Radiofrequency Ablation Therapy for Hepatocellular Carcinoma
- Surgical treatment of bronchobiliary fistula due to radiofrequency ablation for recurrent hepatocellular carcinoma
