J Korean Soc Surg Hand.
2017 Sep;22(3):174-179. 10.12790/jkssh.2017.22.3.174.
Results of Iliac Bone Graft with Kirschner Wire Fixation for Scaphoid Nonunions
- Affiliations
-
- 1Department of Orthopedic Surgery, Sunhan Hospital, Gwangju, Korea.
- 2Department of Orthopedic Surgery, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea. mskim@jnu.ac.kr
- KMID: 2391214
- DOI: http://doi.org/10.12790/jkssh.2017.22.3.174
Abstract
- PURPOSE
To determine clinical and radiographic results of iliac bone grafting with Kirschner wire fixation for treatment of scaphoid nonunions.
METHODS
A total of 13 patients who had scaphoid nonunion treated with iliac bone grafting and Kirschner wire fixation between October 2007 and January 2016 were enrolled as subjects of this study. Their clinical results were evaluated, including range of motion of the wrist joint and modified Mayo wrist score. Radiographic results including lateral intrascaphoid angle and scapholunate angle were also assessed.
RESULTS
Bony union was achieved in 11 (84.6%) of 13 cases. Modified Mayo wrist score was improved from 64.0 preoperatively to 87.5 postoperatively. Average intrascaphoid angle was improved from 39.5° preoperatively to 27.2° postoperatively while scapholunate angle was improved from 66.0° preoperatively to 55.1° postoperatively.
CONCLUSION
Iliac bone graft with Kirschner wire fixation provided good clinical and radiographic results. Therefore, iliac bone graft with Kirschner wire fixation can be considered as a good treatment option for scaphoid nonunion.
Keyword
Figure
-
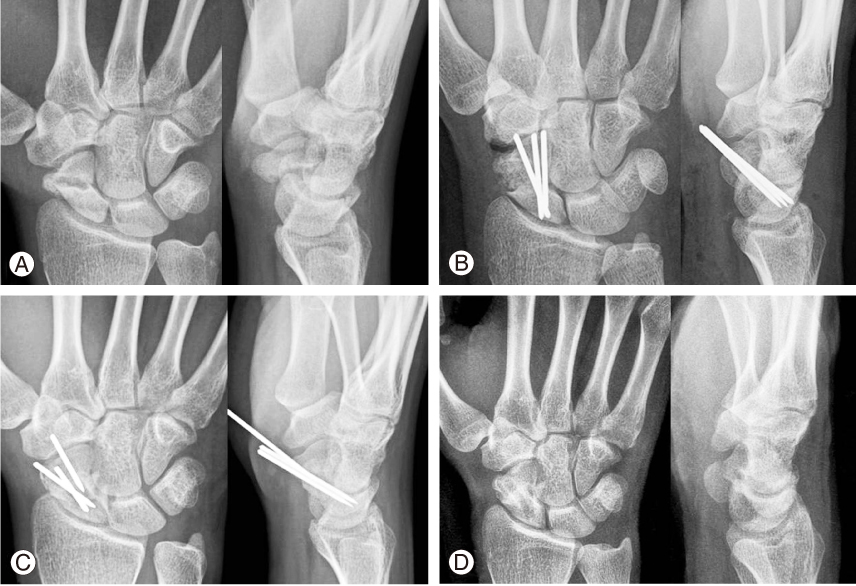
Fig. 1 (A) Preoperative radiograph showing nonunion of the distal third of the scaphoid. (B) Postoperatively radiograph after bone graft and fixation with K-wires. (C) Radiograph at 3 months after surgery showing complete bony union and K-wire migration. (D) Radiograph showing complete bony union after K-wires removal.
Reference
-
1. Cooney WP, Linscheid RL, Dobyns JH. Scaphoid fractures: problems associated with nonunion and avascular necrosis. Orthop Clin North Am. 1984; 15:381–391.2. Mack GR, Bosse MJ, Gelberman RH, Yu E. The natural history of scaphoid non-union. J Bone Joint Surg Am. 1984; 66:504–509.
Article3. Ruby LK, Leslie BM. Wrist arthritis associated with scaphoid nonunion. Hand Clin. 1987; 3:529–539.4. Singh HP, Taub N, Dias JJ. Management of displaced fractures of the waist of the scaphoid: meta-analyses of comparative studies. Injury. 2012; 43:933–939.
Article5. Buijze GA, Ochtman L, Ring D. Management of scaphoid nonunion. J Hand Surg Am. 2012; 37:1095–1100.
Article6. Gabl M, Reinhart C, Lutz M, et al. Vascularized bone graft from the iliac crest for the treatment of nonunion of the proximal part of the scaphoid with an avascular fragment. J Bone Joint Surg Am. 1999; 81:1414–1428.
Article7. Munk B, Larsen CF. Bone grafting the scaphoid nonunion: a systematic review of 147 publications including 5,246 cases of scaphoid nonunion. Acta Orthop Scand. 2004; 75:618–629.8. Trumble T, Nyland W. Scaphoid nonunions: pitfalls and pearls. Hand Clin. 2001; 17:611–624.9. Chen CY, Chao EK, Lee SS, Ueng SW. Osteosynthesis of carpal scaphoid nonunion with interpositional bone graft and Kirschner wires: a 3- to 6-year follow-up. J Trauma. 1999; 47:558–563.
Article10. Tomaino MM, King J, Pizillo M. Correction of lunate malalignment when bone grafting scaphoid nonunion with humpback deformity: rationale and results of a technique revisited. J Hand Surg Am. 2000; 25:322–329.
Article11. Kirkham SG, Millar MJ. Cancellous bone graft and Kirschner wire fixation as a treatment for cavitary-type scaphoid nonunions exhibiting DISI. Hand (N Y). 2012; 7:86–93.
Article12. Panchal A, Kubiak EN, Keshner M, Fulkerson E, Paksima N. Comparison of fixation methods for scaphoid nonunions: a biomechanical model. Bull NYU Hosp Jt Dis. 2007; 65:271–275.13. Stark HH, Rickard TA, Zemel NP, Ashworth CR. Treatment of ununited fractures of the scaphoid by iliac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am. 1988; 70:982–991.
Article14. Christodoulou LS, Kitsis CK, Chamberlain ST. Internal fixation of scaphoid non-union: a comparative study of three methods. Injury. 2001; 32:625–630.
Article15. Finsen V, Hofstad M, Haugan H. Most scaphoid non-unions heal with bone chip grafting and Kirschner-wire fixation. Thirty-nine patients reviewed 10 years after operation. Injury. 2006; 37:854–859.16. Linscheid RL, Dobyns JH, Beabout JW, Bryan RS. Traumatic instability of the wrist: diagnosis, classification, and pathomechanics. J Bone Joint Surg Am. 2002; 84:142.17. Braga-Silva J, Peruchi FM, Moschen GM, Gehlen D, Padoin AV. A comparison of the use of distal radius vascularised bone graft and non-vascularised iliac crest bone graft in the treatment of non-union of scaphoid fractures. J Hand Surg Eur Vol. 2008; 33:636–640.18. Dias JJ. Definition of union after acute fracture and surgery for fracture nonunion of the scaphoid. J Hand Surg Br. 2001; 26:321–325.
Article19. Gupta A, Risitano G, Crawford RJ, Burke FD. The ununited scaphoid:prognostic factors in delayed and nonunions of the scaphoid. Hand Surg. 1999; 4:11–19.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arthroscopic Bone Grafting and Kirschner-Wires Fixation for Scaphoid Nonunion
- Operative Treatment of the Carpal Scaphoid Nonunions
- Treatment of Scaphoid Fractures and Nonunions
- Arthroscopic Bone Grafting and Percutaneous K-Wires Fixation for the Treatment of Scaphoid Nonunion: Surgical Technique
- The Treatnent of Fracture and Nonunion of the Carpal Scaphoid
