Korean J Crit Care Med.
2017 Aug;32(3):247-255. 10.4266/kjccm.2017.00241.
Clinical Application of the Quick Sepsis-Related Organ Failure Assessment Score at Intensive Care Unit Admission in Patients with Bacteremia: A Single-Center Experience of Korea
- Affiliations
-
- 1Department of Internal Medicine, Good Samsun Hospital, Busan, Korea.
- 2Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea. jubilate@pusan.ac.kr
- KMID: 2391184
- DOI: http://doi.org/10.4266/kjccm.2017.00241
Abstract
- BACKGROUND
We evaluated the clinical usefulness of the quick Sepsis-Related Organ Failure Assessment (qSOFA) score (based on the 2016 definition of sepsis) at intensive care unit admission in Korean patients with bacteremia.
METHODS
We retrospectively analyzed clinical data from 236 patients between March 2011 and February 2016. In addition to the qSOFA, the Modified Early Warning score (MEWS) and systemic inflammatory response syndrome (SIRS) criteria were calculated.
RESULTS
The patients' median age was 69 years, and 61.0% were male. Of the patients, 127 (53.8%) had a qSOFA score ≥2 points. They had significantly higher rates of septic shock, thrombocytopenia, and hyperlactatemia, and increased requirements for ventilator care, neuromuscular blocking agents, vasopressors, and hemodialysis within 72 hours after intensive care unit admission. They also had a significantly higher 28-day mortality rate. When analyzed using common thresholds (MEWS ≥5 and ≥2 SIRS criteria), patients with a MEWS ≥5 had the same results as those with a qSOFA score ≥2 (P < 0.05). However, patients with ≥2 SIRS criteria showed no significant differences.
CONCLUSIONS
Our results show that a qSOFA score ≥2 at admission is a useful screening tool for predicting disease severity and medical resource usage within 72 hours after admission, and for predicting 28-day mortality rates in patients with bacteremia. In addition, qSOFA scores may be more useful than SIRS criteria in terms of prognostic utility.
Keyword
MeSH Terms
Figure
-
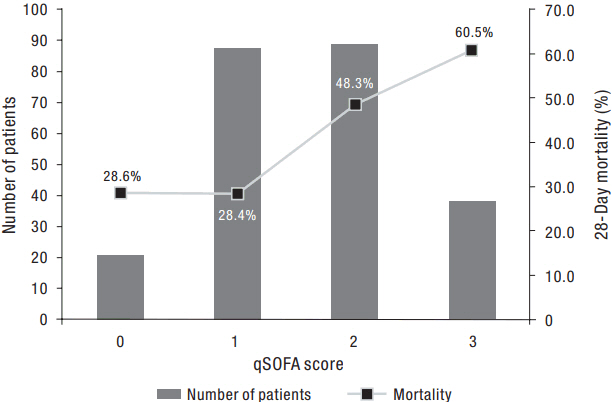
Figure 1. The number of patients for each qSOFA level (left Y axis) and the corresponding mortality (right Y axis). qSOFA: quick Sepsis-Related Organ Failure Assessment.
Reference
-
References
1. Fleischmann C, Scherag A, Adhikari NK, Hartog CS, Tsaganos T, Schlattmann P, et al. Assessment of global incidence and mortality of hospital-treated sepsis: current estimates and limitations. Am J Respir Crit Care Med. 2016; 193:259–72.
Article2. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016; 315:801–10.
Article3. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis: the ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992; 101:1644–55.4. Levy MM, Rhodes A, Phillips GS, Townsend SR, Schorr CA, Beale R, et al. Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Crit Care Med. 2015; 43:3–12.
Article5. Rhodes A, Phillips G, Beale R, Cecconi M, Chiche JD, De Backer D, et al. The Surviving Sepsis Campaign bundles and outcome: results from the International Multicentre Prevalence study on Sepsis (the IMPreSS study). Intensive Care Med. 2015; 41:1620–8.
Article6. Herrán-Monge R, Muriel-Bombín A, García-García MM, Merino-García PA, Cítores-González R, Fernández-Ratero JA, et al. Mortality reduction and long-term compliance with surviving sepsis campaign: a nationwide multicenter study. Shock. 2016; 45:598–606.7. Damiani E, Donati A, Serafini G, Rinaldi L, Adrario E, Pelaia P, et al. Effect of performance improvement programs on compliance with sepsis bundles and mortality: a systematic review and meta-analysis of observational studies. PLoS One. 2015; 10:e0125827.
Article8. Phua J, Koh Y, Du B, Tang YQ, Divatia JV, Tan CC, et al. Management of severe sepsis in patients admitted to Asian intensive care units: prospective cohort study. BMJ. 2011; 342:d3245.
Article9. Kim JH, Hong SK, Kim KC, Lee MG, Lee KM, Jung SS, et al. Influence of full-time intensivist and the nurse-to-patient ratio on the implementation of severe sepsis bundles in Korean intensive care units. J Crit Care. 2012; 27:414.e11–21.
Article10. Kwak SH, Jeong CW, Lee SH, Lee HJ, Koh Y. Current status of intensive care units registered as critical care subspecialty training hospitals in Korea. J Korean Med Sci. 2014; 29:431–7.
Article11. Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. QJM. 2001; 94:521–6.
Article12. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003; 31:1250–6.
Article13. Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013; 39:165–228.
Article14. Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342:1301–8.
Article15. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985; 13:818–29.16. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996; 22:707–10.17. Churpek MM, Snyder A, Han X, Sokol S, Pettit N, Howell MD, et al. Quick Sepsis-Related Organ Failure Assessment, systemic inflammatory response syndrome, and Early Warning Scores for detecting clinical deterioration in infected patients outside the intensive care unit. Am J Respir Crit Care Med. 2017; 195:906–11.
Article18. Williams JM, Greenslade JH, McKenzie JV, Chu K, Brown AFT, Lipman J. Systemic inflammatory response syndrome, quick sequential organ function assessment, and organ dysfunction: insights from a prospective database of ED patients with infection. Chest. 2017; 151:586–96.19. Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens YE, Avondo A, et al. Prognostic accuracy of sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA. 2017; 317:301–8.
Article20. Raith EP, Udy AA, Bailey M, McGloughlin S, MacIsaac C, Bellomo R, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017; 317:290–300.
Article21. Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016; 315:762–74.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lung Injury Score in Predicting the Outcome of the Patients in the Intensive Care Unit
- The Characteristics and Prognostic Factors of Severe Sepsis in Patients Who Were Admitted to a Medical Intensive Care Unit of a Tertiary Hospital
- The quick sepsis-related organ failure score has limited value for predicting adverse outcomes in sepsis patients with liver cirrhosis
- Validation of quick sequential organ failure assessment score for poor outcome prediction among emergency department patients with suspected infection
- Acute Physiology and Chronic Health Evaluation II Score and Sequential Organ Failure Assessment Score as Predictors for Severe Trauma Patients in the Intensive Care Unit
