Korean Circ J.
2017 Sep;47(5):742-751. 10.4070/kcj.2017.0061.
Comparison of Supervised Hospital-based versus Educated Home-based Exercise Training in Korean Heart Failure Patients
- Affiliations
-
- 1Department of Internal Medicine, Heart Institute, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. msk@amc.seoul.kr
- KMID: 2389606
- DOI: http://doi.org/10.4070/kcj.2017.0061
Abstract
- BACKGROUND AND OBJECTIVES
Although many clinical trials have shown that exercise training (ET) improves functional capacity and clinical outcomes in heart failure (HF) patients, data comparing supervised hospital-based and educated home-based ET in HF patients is lacking.
SUBJECTS AND METHODS
This was a single-center, non-randomized, prospective study of 82 HF patients with reduced ejection fraction (≤40%) who completed ET. The hospital-based group (n=30) underwent supervised ET at 60% of peak oxygen consumption (VO₂), while a physiotherapist-educated group (n=52) exercised at home without monitoring. The 2 groups were compared before and after the 3-month ET program with respect to functional capacity, quality of life (QOL), and cardiac events (all-cause mortality or hospitalization with worsening HF).
RESULTS
After ET, peak VOâ‚‚ increased in the hospital-based group (19.4±4.4 to 21.4±4.3 mL/min/kg, p=0.006) and remained unchanged in the home-based group (18.9±4.6 to 18.4±4.6 mL/min/kg, p=0.660). The change in peak VOâ‚‚ after ET was greater in the hospital-based group compared to the home-based group by 2.5 mL/min/kg (p=0.014). QOL improved in the hospital-based group (43.1±18.0 to 28.1±21.6, p=0.003). During one year of follow-up, a comparison of the 2 groups did not reveal a statistical difference in cardiac events (hazard ratio, 0.66; 95% confidence interval, 0.2-2.8; p=0.570).
CONCLUSION
Hospital-based ET was beneficial for HF patients, improving functional capacity and QOL. However, no significant advantages were observed in terms of a composite endpoint compared to home-based ET. Further investigations are required to address the effects and roles of the 2 ET programs for HF patients.
Keyword
MeSH Terms
Figure
-
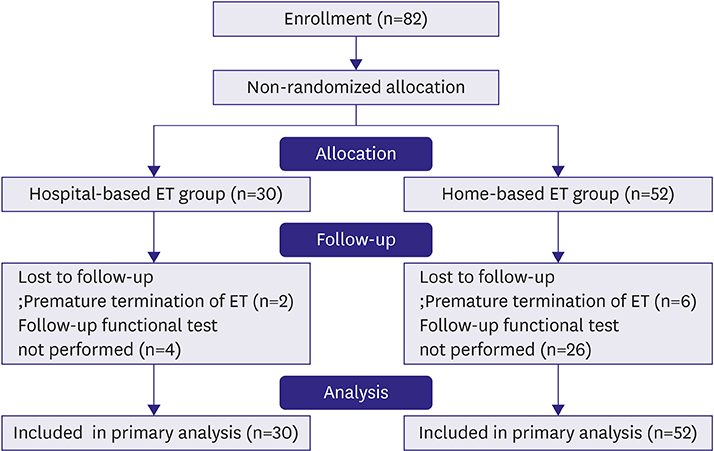
Figure 1 Flow of participants through the trial. ET = exercise training.
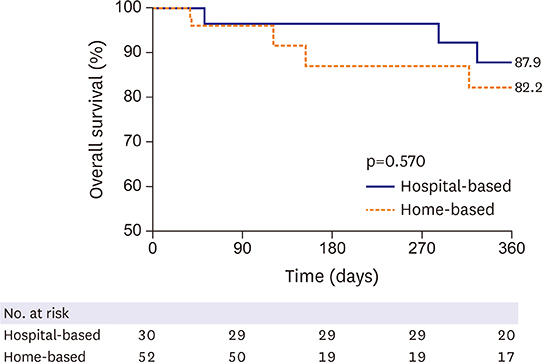
Figure 2 Kaplan-Meier curves for time to composite endpoint (all-cause mortality or hospitalization with worsening HF). The composite endpoint was not statistically different in either group at 1 year after the start of the ET program. ET = exercise training; HF = heart failure.
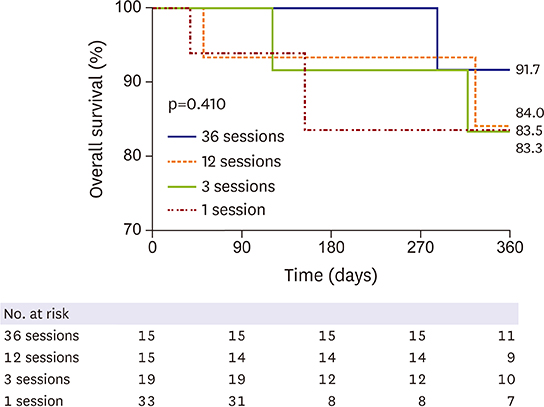
Figure 3 Kaplan-Meier curves for time to composite endpoint (all-cause mortality or hospitalization with worsening HF) by the number of exercise sessions. There was no significant difference between the groups by the number of exercise sessions. HF = heart failure.
Reference
-
1. Lloyd-Jones D, Adams RJ, Brown TM, et al. Executive summary: heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010; 121:948–954.2. Mancini DM, Walter G, Reichek N, et al. Contribution of skeletal muscle atrophy to exercise intolerance and altered muscle metabolism in heart failure. Circulation. 1992; 85:1364–1373.3. Belardinelli R, Georgiou D, Cianci G, Purcaro A. Randomized, controlled trial of long-term moderate exercise training in chronic heart failure: effects on functional capacity, quality of life, and clinical outcome. Circulation. 1999; 99:1173–1182.4. Zwisler AD, Schou L, Soja AM, et al. A randomized clinical trial of hospital-based, comprehensive cardiac rehabilitation versus usual care for patients with congestive heart failure, ischemic heart disease, or high risk of ischemic heart disease (the DANREHAB trial)--design, intervention, and population. Am Heart J. 2005; 150:899.5. O’Connor CM, Whellan DJ, Lee KL, et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA. 2009; 301:1439–1450.6. Mezzani A, Hamm LF, Jones AM, et al. Aerobic exercise intensity assessment and prescription in cardiac rehabilitation: a joint position statement of the European Association for Cardiovascular Prevention and Rehabilitation, the American Association of Cardiovascular and Pulmonary Rehabilitation and the Canadian Association of Cardiac Rehabilitation. Eur J Prev Cardiol. 2013; 20:442–467.7. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013; 62:e147–e239.8. Jessup M, Brozena S. Heart failure. N Engl J Med. 2003; 348:2007–2018.9. Working Group on Cardiac Rehabilitation & Exercice Physiology and Working Group on Heart Failure of the European Society of Cardiology. Recommendations for exercise training in chronic heart failure patients. Eur Heart J. 2001; 22:125–135.10. Hunt SA; American College of Cardiology. American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol. 2005; 46:e1–e82.11. Kim JS, Hwang SY, Shim JL, Jeong MH. Cognitive function and self-care in patients with chronic heart failure. Korean Circ J. 2015; 45:310–316.12. Giannuzzi P, Temporelli PL, Corrà U, Tavazzi L; ELVD-CHF Study Group. Antiremodeling effect of long-term exercise training in patients with stable chronic heart failure: results of the Exercise in Left Ventricular Dysfunction and Chronic Heart Failure (ELVD-CHF) Trial. Circulation. 2003; 108:554–559.13. Demopoulos L, Bijou R, Fergus I, Jones M, Strom J, LeJemtel TH. Exercise training in patients with severe congestive heart failure: enhancing peak aerobic capacity while minimizing the increase in ventricular wall stress. J Am Coll Cardiol. 1997; 29:597–603.14. Lucas C, Stevenson LW, Johnson W, et al. The 6-min walk and peak oxygen consumption in advanced heart failure: aerobic capacity and survival. Am Heart J. 1999; 138:618–624.15. Parnell MM, Holst DP, Kaye DM. Exercise training increases arterial compliance in patients with congestive heart failure. Clin Sci (Lond). 2002; 102:1–7.16. Flynn KE, Piña IL, Whellan DJ, et al. Effects of exercise training on health status in patients with chronic heart failure: HF-ACTION randomized controlled trial. JAMA. 2009; 301:1451–1459.17. Oka RK, De Marco T, Haskell WL, et al. Impact of a home-based walking and resistance training program on quality of life in patients with heart failure. Am J Cardiol. 2000; 85:365–369.18. Wielenga RP, Erdman RA, Huisveld IA, et al. Effect of exercise training on quality of life in patients with chronic heart failure. J Psychosom Res. 1998; 45:459–464.19. Coats AJ, Adamopoulos S, Radaelli A, et al. Controlled trial of physical training in chronic heart failure. Exercise performance, hemodynamics, ventilation, and autonomic function. Circulation. 1992; 85:2119–2131.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Guidelines for Cardiac Rehabilitation
- The Effect of a Self Exercise Program in Cardiac Rehabilitation for Patients with Coronary Artery Disease
- COVID-19, Home Training for Patients with Diabetes Mellitus
- Influence of Home Based Exercise Intensity on the Aerobic Capacity and 1 Year Re-Hospitalization Rate in Patients with Chronic Heart Failure
- Cardiac Rehabilitation of Heart Failure
