J Endocr Surg.
2017 Sep;17(3):89-95. 10.16956/jes.2017.17.3.89.
Loss of the Neuromonitoring Signal on the First Side in Planned Total Thyroidectomy
- Kim HY

- Sun H
- Chai YJ
- Tufano R
- Dralle H
- Navarra G
- Dionigi G
- the Korean Intraoperative Neural Monitoring Society (KINMoS)
- Affiliations
-
- 1KUMC Thyroid Center, Korea University Anam Hospital, Seoul, Korea.
- 2Division of Thyroid Surgery, Jilin Provincial Key Laboratory of Surgical Translational Medicine, China-Japan Union Hospital of Jilin University, Changchun, China. thyroidjl@163.com
- 3Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- 4Department of Otolaryngology-Head and Neck Surgery, The Johns Hopkins University School of Medicine, Baltimore, MD, USA.
- 5Department of General, Visceral, and Transplantation Surgery, University Hospital Essen, Essen, Germany.
- 6Division of Endocrine Surgery, Department of Human Pathology in Adulthood and Childhood “G. Barresiâ€, University Hospital G. Martino, University of Messina, Messina, Italy. gdionigi@unime.it
- KMID: 2389588
- DOI: http://doi.org/10.16956/jes.2017.17.3.89
Abstract
- With an increased use of intraoperative neural monitoring (IONM), an adaptation of the resection strategy appears to be necessary in case of an intraoperative loss of signal (LOS) of the first operated side with total thyroidectomy planned. The contralateral side resection with intact recurrent laryngeal nerve (RLN) function from the surgical point of view, basically has 3 options: 1) no contralateral resection in bilateral goiter, Graves' disease, or low risk thyroid carcinoma (differentiated and medullary thyroid carcinomas) with the aim of 2-stage completion surgery after recovery of nerve function; 2) contralateral subtotal resection ventrally of the RLN plane in benign goiter with a safety distance to the nerve with the aim of avoiding further surgery; and 3) total thyroidectomy as planned for advanced thyroid carcinomas (including undifferentiated thyroid carcinomas) with the aim of immediate postoperative radioiodotherapy. The following document provides a synopsis of the experiences of the Korean Intraoperative Neural Monitoring Society (KINMoS) for the strategy for planned total thyroidectomy and loss of the neuromonitoring signal on the first thyroid lobe.
MeSH Terms
Figure
-
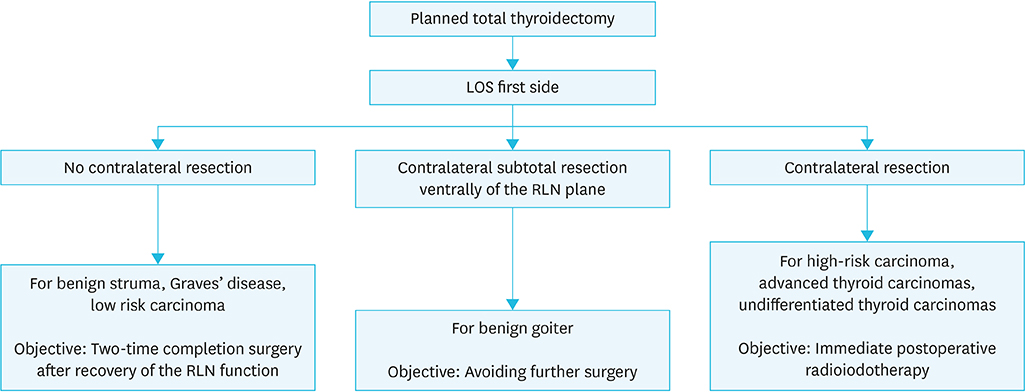
Fig. 1 Surgical options for planned total thyroidectomy and intraoperative signal loss on the first operated side. LOS = loss of signal; RLN = recurrent laryngeal nerve.
Cited by 2 articles
-
It Sometimes Happens: Staging Surgery in Coexisting Graves' Disease and Thyroid Cancer
Ettore Caruso, Maria De Pasquale, Antonella Pino, Vincenzo Bartolo, Fausto Famà, Antonio Ieni, Gianlorenzo Dionigi
J Endocr Surg. 2019;19(3):88-93. doi: 10.16956/jes.2019.19.3.88.Efficacy of Intraoperative Neuromonitoring during Thyroidectomy with Transcutaneous Adhesive Skin Electrodes
Sang Gyu Seo, Hyoung Shin Lee, Ki Hun Jo, Sung Won Kim, Kang Dae Lee
Korean J Otorhinolaryngol-Head Neck Surg. 2021;64(6):416-421. doi: 10.3342/kjorl-hns.2020.00822.
Reference
-
1. Hermann M, Keminger K, Kober F, Nekahm D. Risk factors in recurrent nerve paralysis: a statistical analysis of 7566 cases of struma surgery. Chirurg. 1991; 62:182–187.2. Rosato L, Avenia N, Bernante P, De Palma M, Gulino G, Nasi PG, et al. Complications of thyroid surgery: analysis of a multicentric study on 14,934 patients operated on in Italy over 5 years. World J Surg. 2004; 28:271–276.
Article3. Gilony D, Gilboa D, Blumstein T, Murad H, Talmi YP, Kronenberg J, et al. Effects of tracheostomy on well-being and body-image perceptions. Otolaryngol Head Neck Surg. 2005; 133:366–371.
Article4. Hirano M, Ohala J, Vennard W. The function of laryngeal muscles in regulating fundamental frequency and intensity of phonation. J Speech Hear Res. 1969; 12:616–628.
Article5. Nouraei SA, Whitcroft K, Patel A, Chatrath P, Sandhu GS, Kaddour H. Impact of unilateral vocal fold mobility impairment on laryngopulmonary physiology. Clin Otolaryngol. 2014; 39:210–215.
Article6. Randolph GW, Dralle H; International Intraoperative Monitoring Study Group. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011; 121:Suppl 1. S1–S16.
Article7. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A; German IONM Study Group. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008; 32:1358–1366.
Article8. Hermann M, Hellebart C, Freissmuth M. Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury. Ann Surg. 2004; 240:9–17.9. Schneider R, Lorenz K, Sekulla C, Machens A, Nguyen-Thanh P, Dralle H. Surgical strategy during intended total thyroidectomy after loss of EMG signal on the first side of resection. Chirurg. 2015; 86:154–163.
Article10. Pemberton JD. Exophthalmic goiter: indications for the stage-operation. Arch Surg. 1929; 18:735–744.11. Goretzki PE, Schwarz K, Brinkmann J, Wirowski D, Lammers BJ. The impact of intraoperative neuromonitoring (IONM) on surgical strategy in bilateral thyroid diseases: is it worth the effort? World J Surg. 2010; 34:1274–1284.
Article12. Dralle H, Sekulla C, Lorenz K, Nguyen Thanh P, Schneider R, Machens A. Loss of the nerve monitoring signal during bilateral thyroid surgery. Br J Surg. 2012; 99:1089–1095.
Article13. Sadowski SM, Soardo P, Leuchter I, Robert JH, Triponez F. Systematic use of recurrent laryngeal nerve neuromonitoring changes the operative strategy in planned bilateral thyroidectomy. Thyroid. 2013; 23:329–333.
Article14. Dionigi G, Barczynski M, Chiang FY, Dralle H, Duran-Poveda M, Iacobone M, et al. Why monitor the recurrent laryngeal nerve in thyroid surgery? J Endocrinol Invest. 2010; 33:819–822.
Article15. Henry BM, Graves MJ, Vikse J, Sanna B, Pękala PA, Walocha JA, et al. The current state of intermittent intraoperative neural monitoring for prevention of recurrent laryngeal nerve injury during thyroidectomy: a PRISMA-compliant systematic review of overlapping meta-analyses. Langenbecks Arch Surg. 2017; 402:663–673.
Article16. Barczyński M, Konturek A, Cichoń S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg. 2009; 96:240–246.
Article17. Ho Y, Carr MM, Goldenberg D. Trends in intraoperative neural monitoring for thyroid and parathyroid surgery amongst otolaryngologists and general surgeons. Eur Arch Otorhinolaryngol. 2013; 270:2525–2530.
Article18. Dionigi G, Lombardi D, Lombardi CP, Carcoforo P, Boniardi M, Innaro N, et al. Intraoperative neuromonitoring in thyroid surgery: a point prevalence survey on utilization, management, and documentation in Italy. Updates Surg. 2014; 66:269–276.
Article19. Dralle H, Lorenz K, Machens A. Verdicts on malpractice claims after thyroid surgery: emerging trends and future directions. Head Neck. 2012; 34:1591–1596.
Article20. Schneider R, Randolph GW, Sekulla C, Phelan E, Thanh PN, Bucher M, et al. Continuous intraoperative vagus nerve stimulation for identification of imminent recurrent laryngeal nerve injury. Head Neck. 2013; 35:1591–1598.
Article21. Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010; 34:223–229.
Article22. Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW. The mechanism of recurrent laryngeal nerve injury during thyroid surgery--the application of intraoperative neuromonitoring. Surgery. 2008; 143:743–749.
Article23. Snyder SK, Lairmore TC, Hendricks JC, Roberts JW. Elucidating mechanisms of recurrent laryngeal nerve injury during thyroidectomy and parathyroidectomy. J Am Coll Surg. 2008; 206:123–130.
Article24. Dionigi G, Alesina PF, Barczynski M, Boni L, Chiang FY, Kim HY, et al. Recurrent laryngeal nerve injury in video-assisted thyroidectomy: lessons learned from neuromonitoring. Surg Endosc. 2012; 26:2601–2608.
Article25. Dionigi G, Frattini F. Staged thyroidectomy: time to consider intraoperative neuromonitoring as standard of care. Thyroid. 2013; 23:906–908.
Article26. Melin M, Schwarz K, Lammers BJ, Goretzki PE. IONM-guided goiter surgery leading to two-stage thyroidectomy--indication and results. Langenbecks Arch Surg. 2013; 398:411–418.
Article27. Périé S, Aït-Mansour A, Devos M, Sonji G, Baujat B, St Guily JL. Value of recurrent laryngeal nerve monitoring in the operative strategy during total thyroidectomy and parathyroidectomy. Eur Ann Otorhinolaryngol Head Neck Dis. 2013; 130:131–136.
Article28. Sitges-Serra A, Fontané J, Dueñas JP, Duque CS, Lorente L, Trillo L, et al. Prospective study on loss of signal on the first side during neuromonitoring of the recurrent laryngeal nerve in total thyroidectomy. Br J Surg. 2013; 100:662–666.
Article29. Dionigi G, Boni L, Rovera F, Rausei S, Castelnuovo P, Dionigi R. Postoperative laryngoscopy in thyroid surgery: proper timing to detect recurrent laryngeal nerve injury. Langenbecks Arch Surg. 2010; 395:327–331.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two-Stage Thyroidectomy Driven by Intraoperative Neuromonitoring: Informed Consent Process and Its Effect on Patient Willingness and Consent Rates
- A Case of Minimally Invasive Follicular Thyroid Carcinoma Relapsed as a Large Cervical Lymphadenopathy and Multiple Lung Metastases
- Intraoperative Neuromonitoring during Thyroid Surgery
- It Sometimes Happens: Staging Surgery in Coexisting Graves' Disease and Thyroid Cancer
- The Present and Future of Intraoperative Neuromonitoring in Thyroid Surgery
