Acute Compartment Syndrome Which Causes Rhabdomyolysis by Carbon Monoxide Poisoning and Sciatic Nerve Injury Associated with It: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhang University Gumi Hospital, Gumi, Korea. fovii@naver.com
- KMID: 2389528
- DOI: http://doi.org/10.5371/hp.2017.29.3.204
Abstract
- Rhabdomyolysis is most frequently caused by soft tissue injury with trauma to the extremities. Non-traumatic rhabdomyolysis may be caused by alcohol or drug abuse, infection, collagen disease, or intensive exercise, but incidence is low. In particular, rhabdomyolysis resulting from carbon monoxide poisoning is especially rare. If caught before death, carbon monoxide poisoning has been shown to cause severe muscle necrosis and severe muscle damage leading to acute renal failure. In cases of carbon-monoxide-induced rhabdomyolsis leading to acute compartment syndrome in the buttocks and sciatic nerve injury are rare. We have experience treating patients with acute compartment syndrome due to rhabdomyolysis following carbon monoxide poisoning. We report the characteristic features of muscle necrosis observed during a decompression operation and magnetic resonance imaging findings with a one-year follow-up in addition to a review of the literature.
Keyword
MeSH Terms
-
Acute Kidney Injury
Buttocks
Carbon Monoxide Poisoning*
Carbon Monoxide*
Carbon*
Collagen Diseases
Compartment Syndromes*
Decompression
Extremities
Follow-Up Studies
Humans
Incidence
Magnetic Resonance Imaging
Necrosis
Rhabdomyolysis*
Sciatic Nerve*
Sciatic Neuropathy
Soft Tissue Injuries
Substance-Related Disorders
Carbon
Carbon Monoxide
Figure
-
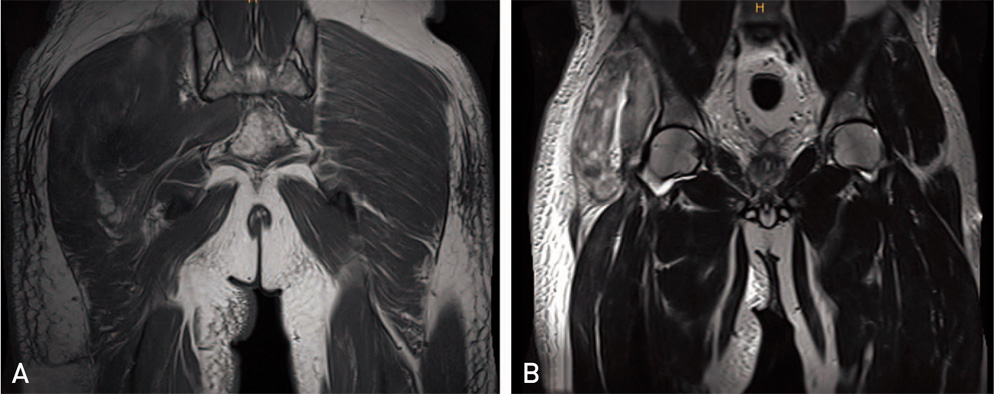
Fig. 1 (A) Axial T1-weighted image shows no enhancement. (B) Coronal T2 weighted image shows heterogenous high signal intensity in the right gluteus maximus, medius, minimus.
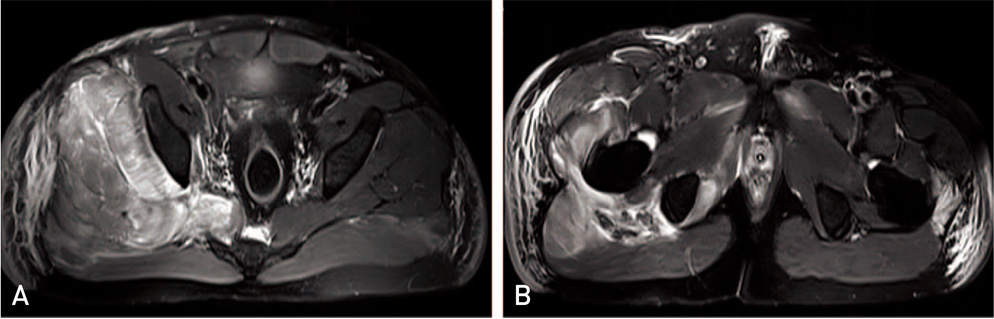
Fig. 2 Axial T2-weighted images show heterogenous high signal intensity in the right gluteus maximus, medius, and minimus. Swelling is especially apparent in the right gluteus medius, and minimus muscles.
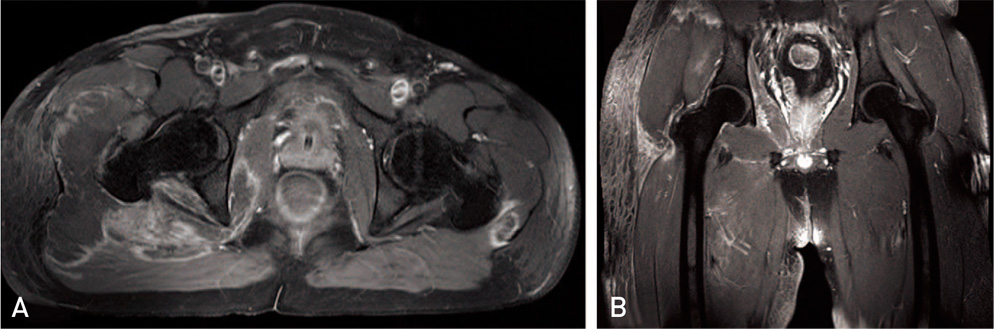
Fig. 3 Axial (A) and coronal (B) gadolinium-enhanced T1-weighted images show faint intramuscular and peripheral enhancement of muscle and subcutaneous fat.

Fig. 4 The results of surgery confirmed the presence of necrotic muscle. Muscle is pale, there was no bleeding, there is no contractility even following electrical stimulation, and there is no elasticity making it easily peeled off with curette.
Cited by 1 articles
-
Immobilization-induced rhabdomyolysis patients with peripheral neuropathy: clinical, laboratory and imaging findings
Jung Im Seok, In Hee Lee, Ki Sung Ahn, Gun Woo Kang, Je Wan Lee, Sanggyu Kwak
Ann Clin Neurophysiol. 2020;22(1):19-23. doi: 10.14253/acn.2020.22.1.19.
Reference
-
1. Lee HY, Lee KH, Han JS, Ahn CR, Kim SG, Lee JS. The Tc-MDP bone scan in the cases of acute renal failure due to carbon monoxide poisoning. Korean J Nephrol. 1985; 4:56–67.2. Chung KJ, Chung YK, Yoo JH, Wang JS. Sciatic nerve palsy complicating gluteal compartment syndrome due to rhabdomyolysis: a case report. J Korean Orthop Assoc. 2005; 40:103–106.
Article3. Thomas MA, Ibels LS. Rhabdomyolysis and acute renal failure. Aust N Z J Med. 1985; 15:623–628.4. Kim HY, Choi SO, Shin SJ, et al. Analysis of 250 cases of rhabdomyolysis. Korean J Nephrol. 1994; 13:810–817.5. Kang SW, Kim YW, Kim YH. Analysis of nontraumatic rhabdo myolysis during recent 2 years. Korean J Med. 2004; 67:467–474.6. Jang SW, Jeon JC, Choi WI. Risk factors associated with complications of carbon monoxide poisoning. J Korean Soc Clin Toxicol. 2009; 7:10–18.7. Owen CA, Woody PR, Mubarak SJ, Hargens AR. Gluteal compartment syndromes: a report of three cases and management utilizing the Wick catheter. Clin Orthop Relat Res. 1978; (132):57–60.8. Jung KC, Kwon ST, Cho KH, Kang SK, Kim JM. MR findings of acute rhabdomyolysis: case report. J Korean Radiol Soc. 2003; 49:119–123.
Article9. Nakahara K, Tanaka H, Masutani K, et al. The value of computed tomography and magnetic resonance imaging to diagnose rhabdomyolysis in acute renal failure. Nephrol Dial Transplant. 1999; 14:1564–1567.
Article10. Kakuda W, Naritomi H, Miyashita K, Kinugawa H. Rhabdomyolysis lesions showing magnetic resonance contrast enhancement. J Neuroimaging. 1999; 9:182–184.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Compartment Syndrome Induced by Carbon Monoxide Poisoning
- Acute Compartment Syndrome in the Pectoral Fascia Due to Prolonged Compression on the Anterior Portion of Left Axilla in C.O. Poisoning: A Case report
- Sciatic Nerve Palsy Complicating Gluteal Compartment Syndrome due to Rhabdomyolysis: A Case Report
- A Case of Rhabdomyolysis Presenting with Acute Kidney Injury Complicating Carbon Monoxide Poisoning
- A Case of Acute Renal Failure Associated with Rhabdomyolysis in Carbon Monoxide Intoxication
