External Snapping Hip Treated by Effective Designed N-plasty of the Iliotibial Band
- Affiliations
-
- 1Department of Orthopaedic Surgery, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. kwj9383@hamail.net
- 2Department of Orthopaedic Surgery, KonKuk University Medical Center, Seoul, Korea.
- 3Department of Orthopaedic Surgery, Soonchunhyang University Seoul Hospital, Seoul, Korea.
- KMID: 2389525
- DOI: http://doi.org/10.5371/hp.2017.29.3.187
Abstract
- PURPOSE
The purpose of this study is to present the effective design of N-plasty of the iliotibial band and surgical results of its use as a treatment for refractory external snapping hip.
MATERIALS AND METHODS
We evaluated 17 patients (24 cases) with external snapping hip who underwent N-plasty between October 2013 and May 2016 and who were followed up for at least 12 months. All patients were male and the mean age was 20.8 years. The mean duration of symptoms prior to surgical intervention was 28.5 months with an average follow up of 24.5 months. Surgery was defined as being successful when patients could carry out their daily activities and exercise without a clicking sensation or pain 6 months after surgery until their last follow-up. Failure was defined when either a clicking sensation or pain was present. The visual analog scale (VAS) and modified Harris hip score (mHHS) were measured and compared preoperatively and at last follow-up.
RESULTS
All patients had complete resolution of pain and snapping. The VAS decreased from 6.77 preoperatively to 0.09 postoperatively and mHHS improved from 69.5 to 97.8 after surgery.
CONCLUSION
Modified designed N-plasty is considered to be an excellent treatment method facilitating operation reproducibility with maximum elongation effect of the iliotibial band.
Keyword
Figure
-
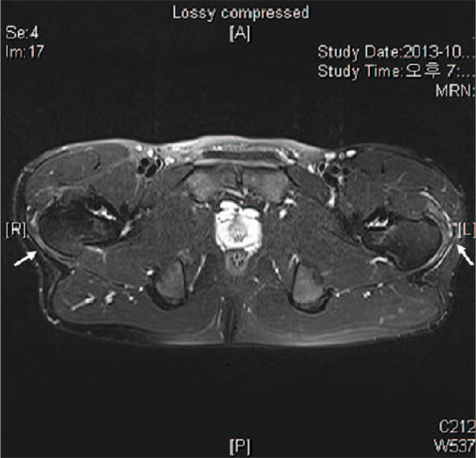
Fig. 1 Magnetic resonance imaging (MRI) examinations. A 21-year-old man with bilateral snapping hip syndrome. The T2-weighted MRI of both hips show thickening and fibrosis of the iliotibial band and greater trochanteric bursitis (arrows).

Fig. 2 Diagram of N-plasty design by Yi et al.1) shows incision and transposition of iliotibial band. (A) Proximal flap and distal flap are determined. (B) Proximal flap is sutured cross with distal flap. (C) Suture is performed at each incision edge. (D) Iliotibial band could be lengthened and narrowed.
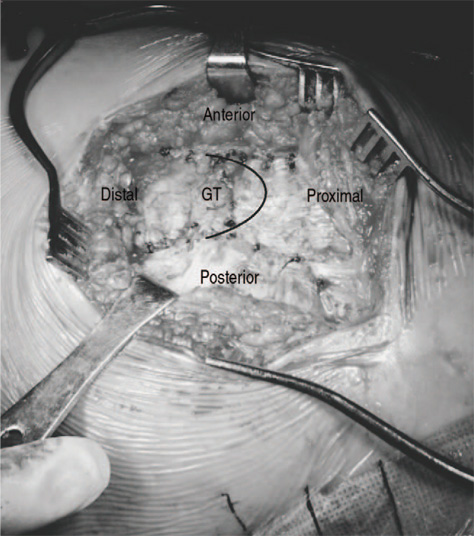
Fig. 3 Clinical photogragh shows the figure of N-plasty on the iliotibial band. GT: greater trochanter.
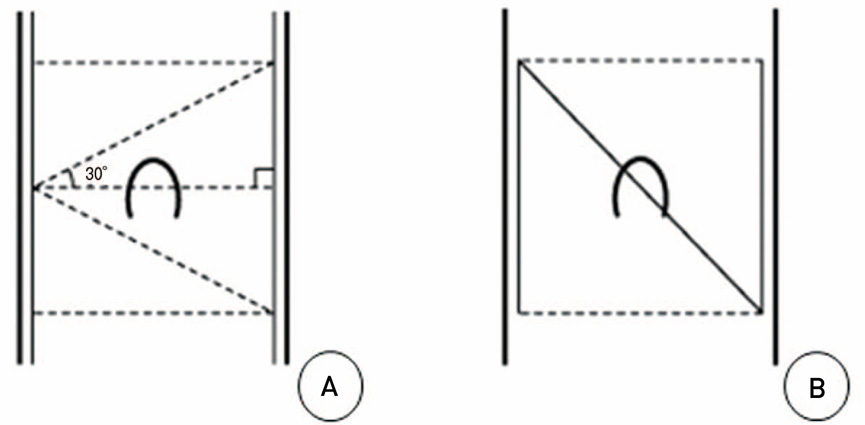
Fig. 4 (A) Anterior and posterior margin lengths are determined by drawing lines from the anterior margin at the area of greater trochanter to proximal and distal portion of posterior margin with 30° of angle each. (B) Design of the N-plasty is accomplished by determined length of the anterior and posterior margin.
Reference
-
1. Yi SR, Lee SH, No JH, Park JM. The surgical treatment of external snapping hip by modified Z-plasty (N-plasty) of the iliotibial band. J Korean Hip Soc. 2008; 20:315–319.
Article2. Allen WC, Cope R. Coxa saltans: the snapping hip revisited. J Am Acad Orthop Surg. 1995; 3:303–308.
Article3. Yi SR, Kim SW, Song J. Surgical treatment of snapping hip by modified Z-plasty of the iliotibial band. Korean J Sports Med. 2012; 30:144–147.
Article4. Brignall CG, Stainsby GD. The snapping hip. Treatment by Z-plasty. J Bone Joint Surg Br. 1991; 73:253–254.
Article5. Larsen E, Johansen J. Snapping hip. Acta Orthop Scand. 1986; 57:168–170.
Article6. Zoltan DJ, Clancy WG Jr, Keene JS. A new operative approach to snapping hip and refractory trochanteric bursitis in athletes. Am J Sports Med. 1986; 14:201–204.
Article7. Teitz CC, Garrett WE Jr, Miniaci A, Lee MH, Mann RA. Tendon problems in athletic individuals. Instr Course Lect. 1997; 46:569–582.8. Brignall CG, Brown RM, Stainsby GD. Fibrosis of the gluteus maximus as a cause of snapping hip. A case report. J Bone Joint Surg Am. 1993; 75:909–910.
Article9. Nam KW, Yoo JJ, Koo KH, Yoon KS, Kim HJ. A modified Z-plasty technique for severe tightness of the gluteus maximus. Scand J Med Sci Sports. 2011; 21:85–89.
Article10. Battaglia M, Guaraldi F, Monti C, Vanel D, Vannini F. An unusual cause of external snapping hip. J Radiol Case Rep. 2011; 5:1–6.
Article11. Lin CL, Huang MT, Lin CJ. Snapping hip caused by a venous hemangioma of the gluteus maximus muscle: a case report. J Med Case Rep. 2008; 2:386.
Article12. Gopisankar Balaji G, Patil NK, Menon J. Coxa saltans caused by extraarticular synovial chondromatosis overlying an isolated osteochondroma of the greater trochanter: A rare aetiology. J Clin Orthop Trauma. 2015; 6:126–130.
Article13. Larsen E, Gebuhr P. Snapping hip after total hip replacement. A report of four cases. J Bone Joint Surg Am. 1988; 70:919–920.
Article14. Brooker AF Jr. The surgical approach to refractory trochanteric bursitis. Johns Hopkins Med J. 1979; 145:98–100.15. Féry A, Sommelet J. [The snapping hip. Late results of 24 surgical cases]. Int Orthop. 1988; 12:277–282. French.16. White RA, Hughes MS, Burd T, Hamann J, Allen WC. A new operative approach in the correction of external coxa saltans: the snapping hip. Am J Sports Med. 2004; 32:1504–1508.
Article17. Ilizaliturri VM Jr, Martinez-Escalante FA, Chaidez PA, Camacho-Galindo J. Endoscopic iliotibial band release for external snapping hip syndrome. Arthroscopy. 2006; 22:505–510.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Snapping Hip by Modified Z-plasty of the Iliotibial Band
- The Surgical Treatment of External Snapping Hip by Modified Z-plasty (N-plasty) of the Iliotibial Band
- External Snapping Hip Syndrome: Emphasis on the MR Imaging
- Arthroscopic Treatment for External Snapping Hip
- Snapping Knee caused by the Semitendinous Tendon: A Case Report
