Joubert Syndrome Presenting With Normal Pyramidal Decussation: A Case Report
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Chonbuk National University Medical School, Jeonju, Korea. shpark0130@jbnu.ac.kr
- KMID: 2389417
- DOI: http://doi.org/10.5535/arm.2017.41.4.701
Abstract
- Joubert syndrome (JS) is a rare genetic disorder characterized by a congenital malformation of the hindbrain, and accompanied by axonal decussation abnormalities affecting the corticospinal tract and the superior cerebellar peduncles. To the best of our knowledge, there are no reports of normal pyramidal decussation in JS. Here, we describe the case of an 18-year-old boy presenting midline-crossing corticospinal projections, which were considered normal corticospinal tract trajectories. Diffusion tensor imaging and motor evoked potential study analysis demonstrated the exclusive presence of decussating corticospinal projections in the patient. Based on these results, we suggest that JS might be associated with several, diverse corticospinal motor tract organization patterns.
MeSH Terms
Figure
-
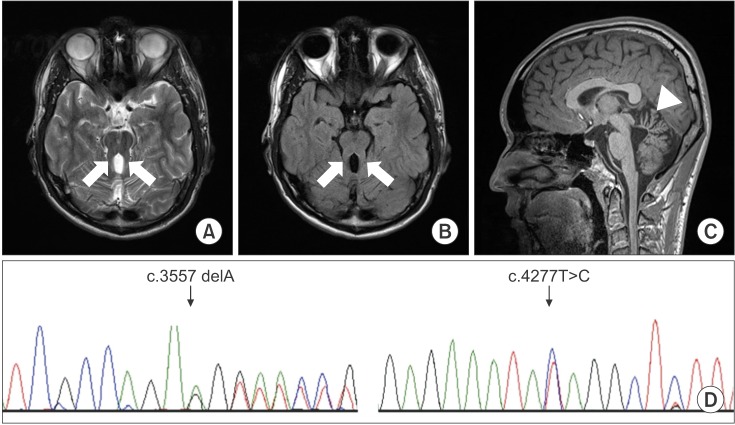
Fig. 1 Axial T2-weighted (A) and T2-weighted fluid-attenuated inversion recovery (B) brain magnetic resonance imaging scans at the pontomesencephalic junction show the molar tooth sign (arrow). The midsagittal T1-weighted image (C) shows hypoplasia of the cerebellar vermis (arrowhead). Sanger sequencing chromatograms verified c.3557delA and c.4277T>C in the C5orf42 gene (D). The black indicates a guanine, red indicates a thymine, blue indicates a cytosine, and green indicates an adenine.
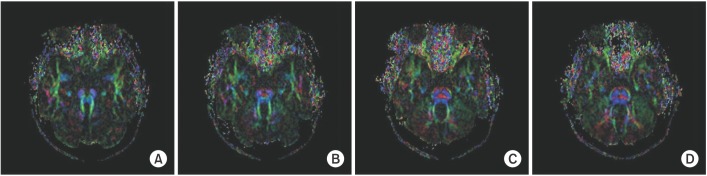
Fig. 2 Axial color-coded map at the level of the pontomesencephalic junction shows the absence of the midline ‘focal red dot’ which is interpreted as the absent decussation of the fiber tracts within the superior cerebellar peduncles (A). The transpontine fiber shows no abnormality at the basis pontis (B, C, D). The red indicates a predominant left-right (x-element), green indicates an anteroposterior (y-element), and blue indicates a superior-inferior (z-element) orientation of the anisotropic component of diffusion within each voxel.
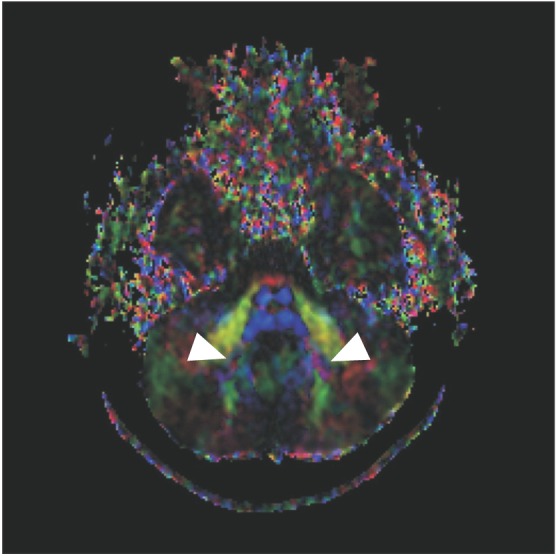
Fig. 3 Diffuse tensor imaging at the level of the dentate nuclei shows that the dentate nuclei is abnormally located more laterally (arrowheads).
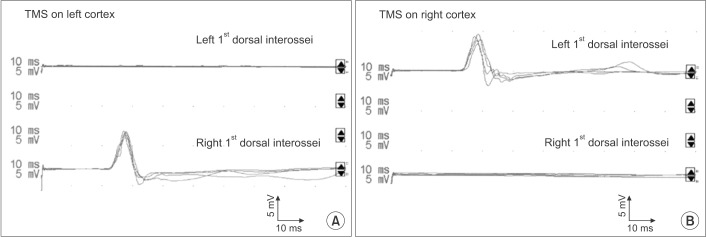
Fig. 4 Recording of the right and left 1st dorsal interossei motor evoked potentials with transcranial magnetic stimulation of left (A) and right (B) cortex shows contralateral responses only, suggesting crossed corticospinal projections from each hemisphere. TMS, transcranial magnetic stimulation.
Reference
-
1. Maria BL, Boltshauser E, Palmer SC, Tran TX. Clinical features and revised diagnostic criteria in Joubert syndrome. J Child Neurol. 1999; 14:583–590. PMID: 10488903.
Article2. Yachnis AT, Rorke LB. Neuropathology of Joubert syndrome. J Child Neurol. 1999; 14:655–659. PMID: 10511338.
Article3. Poretti A, Boltshauser E, Loenneker T, Valente EM, Brancati F, Il'yasov K, et al. Diffusion tensor imaging in Joubert syndrome. AJNR Am J Neuroradiol. 2007; 28:1929–1933. PMID: 17898198.
Article4. Theoret H, Gleeson J, Pascual-Leone A. Neurophysiologic characterization of motor and sensory projections in Joubert syndrome. Clin Neurophysiol. 2013; 124:2283–2284. PMID: 23906682.5. Srour M, Schwartzentruber J, Hamdan FF, Ospina LH, Patry L, Labuda D, et al. Mutations in C5ORF42 cause Joubert syndrome in the French Canadian population. Am J Hum Genet. 2012; 90:693–700. PMID: 22425360.
Article6. Schutta HS, Abu-Amero KK, Bosley TM. Exceptions to the Valsalva doctrine. Neurology. 2010; 74:329–335. PMID: 20101039.
Article7. Parisi MA, Pinter JD, Glass IA, Field K, Maria BL, Chance PF, et al. Cerebral and cerebellar motor activation abnormalities in a subject with Joubert syndrome: functional magnetic resonance imaging (MRI) study. J Child Neurol. 2004; 19:214–218. PMID: 15119482.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Neonatal Onset Joubert Syndrome
- Atlanto-Axial Dislocation with Odontoid Process Fracture Associated with "Cruciate Paralysis"
- A Case of Joubert Syndrome Associated with Nephrocalcinosis and Agenesis of Cerebellar Vermis
- Joubert Syndrome with Severe Hypotonia: A case report
- Joubert Syndrome Presented with Ocular Motor Apraxia
