Back Extensor Strengthening Exercise and Backpack Wearing Treatment for Camptocormia in Parkinson's Disease: A Retrospective Pilot Study
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, National Health Insurance Service Ilsan Hospital, Goyang, Korea. rehappydoc@gmail.com
- KMID: 2389414
- DOI: http://doi.org/10.5535/arm.2017.41.4.677
Abstract
OBJECTIVE
To investigate the effect of a conservative treatment regime in Parkinson's disease patients with camptocormia.
METHODS
Nine patients with Parkinson's disease were included in a retrospective pilot study of the value of back extensor strengthening exercise. Six inpatients received a 30-minute treatment, twice daily for 5 weeks, being treated on average for 34 days; while three outpatients visited the clinic and were educated for home exercise and backpack wearing treatment. Outpatients should be scheduled to visit the outpatient department to check physical status every 2-4 weeks for an average of 3 months.
RESULTS
All patients except one showed statistically significant improvements in activities of daily living (ADL) and motor symptoms, as measured by flexion angle at standing posture, Unified Parkinson's Disease Rating Scale (UPDRS) II and III, and modified Hoehn-Yahr staging.
CONCLUSION
Conservative treatment is effective in postural correction of camptocormia in Parkinson's disease, as well as improvement in ADL and motor symptoms.
MeSH Terms
Figure
-
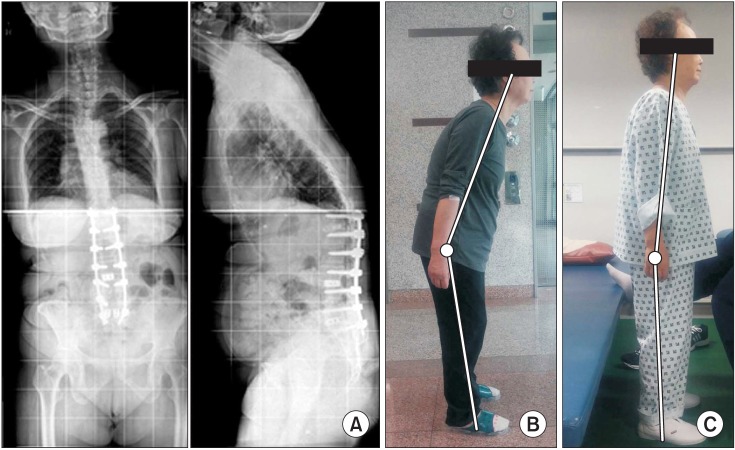
Fig. 1 Patient #7 before and after treatment. (A) She had an operative treatment for kyphosis and lower back pain but showed camptocormia afterwards. (B) Lateral image before rehabilitation treatment. (C) Lateral image after rehabilitation treatment.
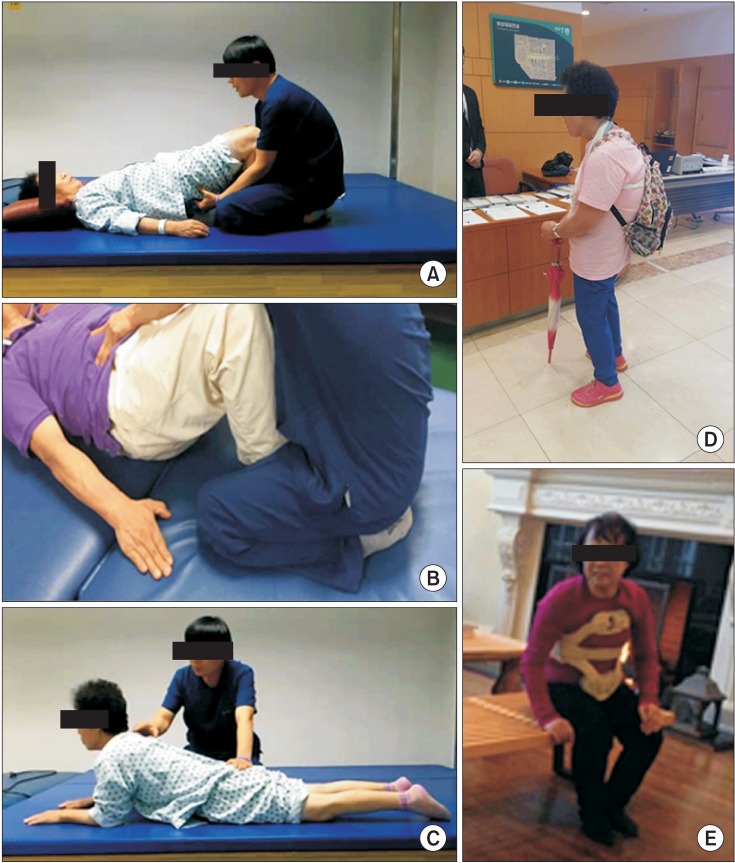
Fig. 2 Various modalities of conservative management for camptocormia. (A) Core muscle strengthening exercise. (B) Pelvic tilting exercise. (C) Back extensor strengthening exercise. (D) Low-slung backpack. (E) Anterior spinal hyperflexion brace.
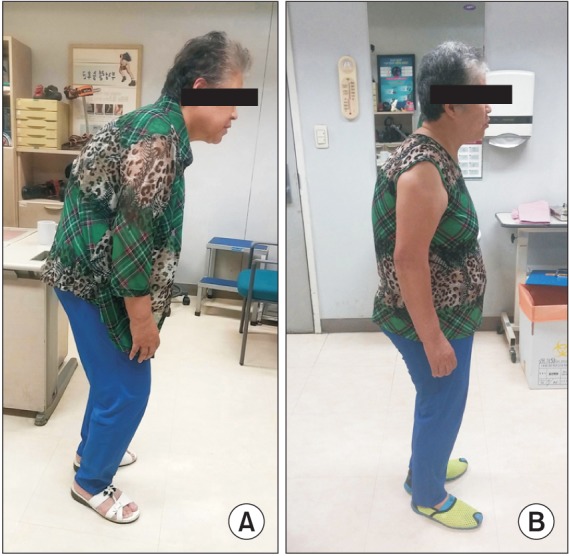
Fig. 3 Patient #4 before and after treatment. She was educated for home exercise at the outpatient clinic. After 4 weeks of home exercise and low-slung backpack treatment, she showed improvement of camptocormia. (A) Lateral image before rehabilitation treatment. (B) Lateral image after rehabilitation treatment.
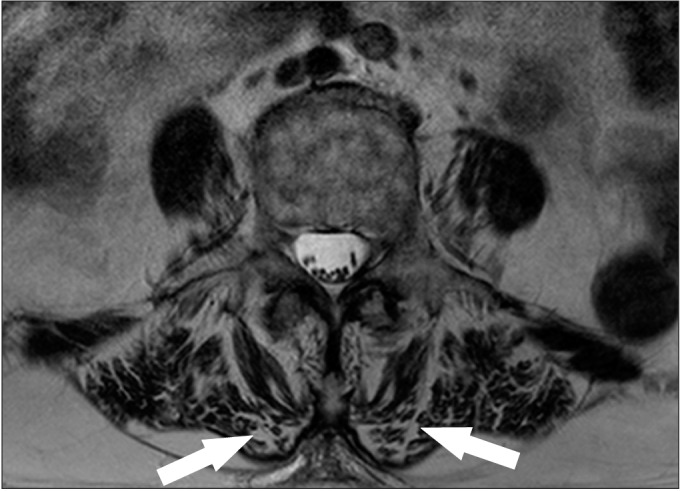
Fig. 4 Lumbar spine magnetic resonance imaging of patient #1. The arrows indicate atrophic change of paraspinal muscle in magnetic resonance imaging T2 image of patient #1.

Fig. 5 Increased angle of camptocormia during ambulation of patient #9. (A) At the beginning, angle of camptocormia is smaller. (B) After 10 minutes of gait, angle of camptocormia increased.
Reference
-
1. Asahi T, Taguchi Y, Hayashi N, Hamada H, Dougu N, Takashima S, et al. Bilateral subthalamic deep brain stimulation for camptocormia associated with Parkinson's disease. Stereotact Funct Neurosurg. 2011; 89:173–177. PMID: 21494070.
Article2. Seki M, Takahashi K, Koto A, Mihara B, Morita Y, Isozumi K, et al. Camptocormia in Japanese patients with Parkinson's disease: a multicenter study. Mov Disord. 2011; 26:2567–2571. PMID: 21953897.
Article3. Tiple D, Fabbrini G, Colosimo C, Ottaviani D, Camerota F, Defazio G, et al. Camptocormia in Parkinson disease: an epidemiological and clinical study. J Neurol Neurosurg Psychiatry. 2009; 80:145–148. PMID: 18931011.
Article4. Srivanitchapoom P, Hallett M. Camptocormia in Parkinson's disease: definition, epidemiology, pathogenesis and treatment modalities. J Neurol Neurosurg Psychiatry. 2016; 87:75–85. PMID: 25896683.
Article5. Azher SN, Jankovic J. Camptocormia: pathogenesis, classification, and response to therapy. Neurology. 2005; 65:355–359. PMID: 16087897.
Article6. Ye BK, Kim HS, Kim YW. Correction of camptocormia using a cruciform anterior spinal hyperextension brace and back extensor strengthening exercise in a patient with Parkinson disease. Ann Rehabil Med. 2015; 39:128–132. PMID: 25750882.
Article7. Colosimo C, Salvatori FM. Injection of the iliopsoas muscle with botulinum toxin in camptocormia. Mov Disord. 2009; 24:316–317. PMID: 18973251.
Article8. Bloch F, Houeto JL, Tezenas du Montcel S, Bonneville F, Etchepare F, Welter ML, et al. Parkinson's disease with camptocormia. J Neurol Neurosurg Psychiatry. 2006; 77:1223–1228. PMID: 16754693.
Article9. Doherty KM, van de Warrenburg BP, Peralta MC, Silveira-Moriyama L, Azulay JP, Gershanik OS, et al. Postural deformities in Parkinson's disease. Lancet Neurol. 2011; 10:538–549. PMID: 21514890.
Article10. von Coelln R, Raible A, Gasser T, Asmus F. Ultrasound-guided injection of the iliopsoas muscle with botulinum toxin in camptocormia. Mov Disord. 2008; 23:889–892. PMID: 18307265.
Article11. Yamada K, Goto S, Matsuzaki K, Tamura T, Murase N, Shimazu H, et al. Alleviation of camptocormia by bilateral subthalamic nucleus stimulation in a patient with Parkinson's disease. Parkinsonism Relat Disord. 2006; 12:372–375. PMID: 16731023.
Article12. Capelle HH, Schrader C, Blahak C, Fogel W, Kinfe TM, Baezner H, et al. Deep brain stimulation for camptocormia in dystonia and Parkinson's disease. J Neurol. 2011; 258:96–103. PMID: 20803027.
Article13. Hellmann MA, Djaldetti R, Israel Z, Melamed E. Effect of deep brain subthalamic stimulation on camptocormia and postural abnormalities in idiopathic Parkinson's disease. Mov Disord. 2006; 21:2008–2010. PMID: 16972244.
Article14. Umemura A, Oka Y, Ohkita K, Yamawaki T, Yamada K. Effect of subthalamic deep brain stimulation on postural abnormality in Parkinson disease. J Neurosurg. 2010; 112:1283–1288. PMID: 19895200.
Article15. Thani NB, Bala A, Kimber TE, Lind CR. High-frequency pallidal stimulation for camptocormia in Parkinson disease: case report. Neurosurgery. 2011; 68:E1501–E1505. PMID: 21307785.
Article16. Sako W, Nishio M, Maruo T, Shimazu H, Matsuzaki K, Tamura T, et al. Subthalamic nucleus deep brain stimulation for camptocormia associated with Parkinson's disease. Mov Disord. 2009; 24:1076–1079. PMID: 19353719.
Article17. Upadhyaya CD, Starr PA, Mummaneni PV. Spinal deformity and Parkinson disease: a treatment algorithm. Neurosurg Focus. 2010; 28:E5.
Article18. Gerton BK, Theeler B, Samii A. Backpack treatment for camptocormia. Mov Disord. 2010; 25:247–248. PMID: 20077473.
Article19. Schroeteler FE, Fietzek UM, Ziegler K, Ceballos-Baumann AO. Upright posture in parkinsonian camptocormia using a high-frame walker with forearm support. Mov Disord. 2011; 26:1560–1561. PMID: 21520281.
Article20. de Seze MP, Creuze A, de Seze M, Mazaux JM. An orthosis and physiotherapy programme for camptocormia: a prospective case study. J Rehabil Med. 2008; 40:761–765. PMID: 18843430.
Article21. Capecci M, Serpicelli C, Fiorentini L, Censi G, Ferretti M, Orni C, et al. Postural rehabilitation and Kinesio taping for axial postural disorders in Parkinson';s disease. Arch Phys Med Rehabil. 2014; 95:1067–1075. PMID: 24508531.
Article22. Schulz-Schaeffer WJ, Margraf NG, Munser S, Wrede A, Buhmann C, Deuschl G, et al. Effect of neurostimulation on camptocormia in Parkinson's disease depends on symptom duration. Mov Disord. 2015; 30:368–372. PMID: 25678310.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction of Camptocormia Using a Cruciform Anterior Spinal Hyperextension Brace and Back Extensor Strengthening Exercise in a Patient With Parkinson Disease
- Effect of Lumbar Extensor Strengthening in Chronic Low Back Pain Patients
- The Effect of Back Extensor Strengthening Exercise on Chronic Low Back Pain and Bone Mineral Density
- Comparisons of Spinal Stabilization Exercise and Lumbar Extensor Strengthening Exercise in Chronic Low Back Pain
- Effects of Lumbar Strengthening Exercise in Lower-Limb Amputees With Chronic Low Back Pain
