Mechanical Extraction of a Massive Intracoronary Thrombus from the Super-Dominant Right Coronary Artery in Thrombogenic Lung Cancer Patient
- Affiliations
-
- 1Division of Cardiology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. jo1216@inje.ac.kr
- 2Department of Radiology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2389134
- DOI: http://doi.org/10.4070/kcj.2015.45.3.248
Abstract
- The congenital absence of the left circumflex artery and a compensatory super-dominant right coronary artery (RCA) is a very rare benign coronary anomaly in the clinic. The presence of a massive thrombus in the super-dominant RCA can lead to fatal results in cases of acute myocardial infarction, unless the thrombus is mechanically removed. Aspiration of the thrombus using a 6 Fr right Judkins guide catheter is useful to extract a massive thrombus and is both safe and effective. We report a case of complete revascularization of the super-dominant RCA after thrombus aspiration using a 6 Fr Judkins right catheter in a patient with acute inferior and inferolateral wall myocardial infarction.
MeSH Terms
Figure
-
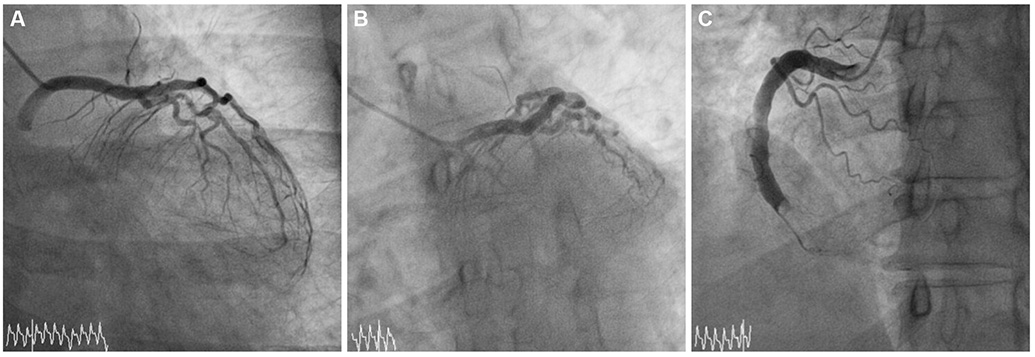
Fig. 1 Baseline coronary angiogram. A and B: the left circumflex artery is not seen in both caudal view and left-anterior-oblique with caudal view of the left coronary angiogram. C: massive thrombotic occlusion in super-dominant right coronary artery is noted on the right coronary angiogram.

Fig. 2 Coronary thrombus aspiration with 6 Fr guide catheter. A: the Judkins right guide catheter (arrow) can be deeply positioned into the super-dominant right coronary artery using a clock-wise rotation. B: the massive fresh thrombus is successfully removed by direct catheter aspiration.
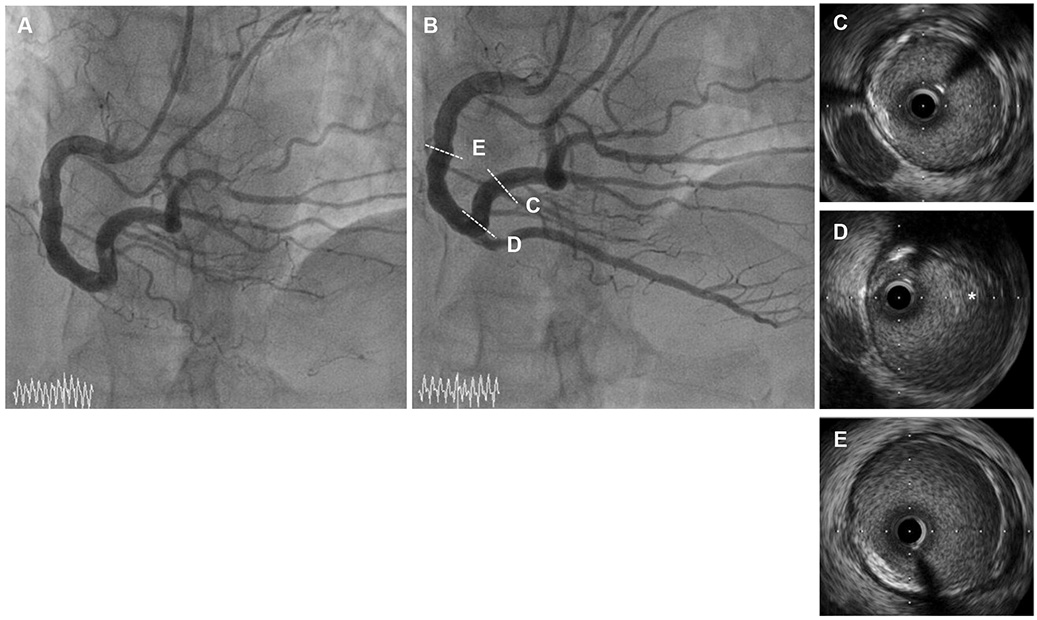
Fig. 3 Final coronary angiogram and repeated coronary angiogram. A: after the effective extraction of the massive thrombus, distal trees of the right coronary artery appears and extends to the territory of the left circumflex artery. B: remnant intracoronary thrombus almost disappears after continuous intravenous administration of unfractionated heparin for eight days. C, D, and E: atheromatous plaque or ruptured plaque is not observed on the intravascular ultrasound. *small remnant thrombus.

Fig. 4 An acute pulmonary thromboembolism develops two weeks after discharge under dual antiplatelet therapy with no evidence of hypercoagulopathies. A chest CT scan shows intra-arterial emboli (arrows) in the right lower basal segmental pulmonary arteries.
Reference
-
1. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990; 21:28–40.2. Gentzler RD 2nd, Gault JH, Liedtke AJ, McCann WD, Mann RH, Hunter AS. Congenital absence of the left circumflex coronary artery in the systolic click syndrome. Circulation. 1975; 52:490–496.3. Bestetti RB, Costa RB, Oliveira JS, Rossi MA, Corrêa de. Congenital absence of the circumflex coronary artery associated with dilated cardiomyopathy. Int J Cardiol. 1985; 8:331–335.4. Guo J, Xu M. Congenital absence of the left circumflex artery associated with inferior myocardial infarction. Intern Med. 2012; 51:71–74.5. Hong PS, Lee YS, Lee JB. Congenital absence of the left circumflex coronary artery in a patient with acute inferior myocardial infarction. Herz. 2014; 39:957–959.6. Farto e Abreu P, Mesquita A, Silva JA, Seabra-Gomes R. [Coronary artery ectasia: clinical and angiographic characteristics and prognosis]. Rev Port Cardiol. 1993; 12:305–310.7. van Ooijen PM, Dorgelo J, Zijlstra F, Oudkerk M. Detection, visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol. 2004; 14:2163–2171.8. Yip HK, Wu CJ, Chang HW, et al. Comparison of impact of primary percutaneous transluminal coronary angioplasty and primary stenting on short-term mortality in patients with cardiogenic shock and evaluation of prognostic determinants. Am J Cardiol. 2001; 87:1184–1188.9. Rath S, Har-Zahav Y, Battler A, et al. Fate of nonobstructive aneurysmatic coronary artery disease: angiographic and clinical follow-up report. Am Heart J. 1985; 109:785–791.10. Onoda S, Mutoh M, Ishikawa T, et al. Usefulness of a 6 fr right judkins catheter for mechanically extracting a massive intracoronary thrombus from an ectasic right coronary artery: a report on two different cases of thrombectomy. Jpn Heart J. 2004; 45:673–678.11. Hara M, Saikawa T, Tsunematsu Y, Sakata T, Yoshimatsu H. Predicting no-reflow based on angiographic features of lesions in patients with acute myocardial infarction. J Atheroscler Thromb. 2005; 12:315–321.12. Fujii T, Ueda M, Ikura Y, et al. Aspirated intracoronary thrombus by Rescue™ PT catheter (histological and immunohistochemical analyses). Circulation. 2002; 66:Suppl. I–458.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of a Successful Percutaneous Coronary Intervention Using Percusurge(r) System in a Massive Intracoronary Thrombi Patient
- No-Reflow Phoenomenon by Intracoronary Thrombus in Acute Myocardial Infarction
- Intracoronary Thrombolysis and Delayed Percutaneous Coronary Intervention for the Treatment of Large Coronary Thrombi in a Patient with Polycythemia Vera
- A Case of Treatment of Acute Occlusion Complicating Percutaneous Transluminal Coronary Angioplasty
- Aspiration Thromboembolectomy in the Management of Acute Coronary Occlusion during Pertaneous Transluminal Coronary Angioplasty
