Small Left Atrial Size Complicating Percutaneous Transcatheter Device Closure of Secundum Atrial Septal Defect with Conventional Approach
- Affiliations
-
- 1Department of Pediatrics, Ajou University Hospital, Ajou University School of Medicine, Suwon, Korea.
- 2Division of Pediatric Cardiology, Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. yhkim@amc.seoul.kr
- KMID: 2389129
- DOI: http://doi.org/10.4070/kcj.2015.45.3.216
Abstract
- BACKGROUND AND OBJECTIVES
Transcatheter device closure becomes the first option for treating secundum atrial septal defect (ASD), but the conventional method is sometimes unsuccessful even when the defect size indicates the closure to be feasible. To increase the success rate, modified methods have been introduced and used. This study aimed to find predictors for using the modified methods in the device closure of secundum ASDs.
SUBJECTS AND METHODS
Between October 2010 and December 2012, 92 patients with ASDs underwent the transcatheter device closure. We analyzed the sizes of the defect, the surrounding rims, and the ratios of the left atrium (LA) dimensions to the device size in the patients who underwent the procedure either using the conventional or modified methods.
RESULTS
Among the 88 successful cases (95.7%), 22 patients (25%) required modified methods (12 using pulmonary vein and 10 using balloon). The modified method group had the larger size of ASDs and smaller posterosuperior rim. The mean ratios of the LA anteroposterior diameter, width, and length to the device size were all significantly smaller in the modified methods group than in the conventional group (1.20 vs. 1.56, 1.32 vs. 1.71, and 1.61 vs. 2.07, respectively). We found that the risk factors for the modified methods were smaller retroaortic rim, larger ASD, and smaller LA dimension/device size.
CONCLUSION
In addition to larger defects and smaller retroaortic rim, the smaller ratios of the LA dimensions to the device size influenced the need for the application of modified methods in the transcatheter device closure of ASDs.
Keyword
MeSH Terms
Figure
-

Fig. 1 Measurements of the LA diameters (A, B, C) and schematic diagram of the surrounding rims from the pre-interventional TTE (D). A: AP, anteroposterior diameter measured at the midline of the LA from a PLAX view during an end-systolic phase (red). B: parameters measured from an A4C view at an end systolic phase; W, width (blue); LA4C, length (yellow); AA4C, area measured from an A4C view (sky blue). C: parameters measured from an A2C at an end systolic phase; LA2C, length (yellow); AA2C, area measured from an A2C (sky blue). D: gray regions represent the surrounding rims measured from a subcoastal, an A4C, and a PSAX view. LA: left atrium, TTE: transthoracic echocardiography, PLAX: parasternal long axis, A4C: apical four chambers, A2C: apical two chambers, PSAX: parasternal short axis, FR: frame rate, C: compression rate, P: persistent grade, HGen: general harmony, BPM: beat per minute, ASD: secundum atrial septal defect, TV: tricuspid valve.

Fig. 2 Pulmonary vein method and schematic diagram. Angiographic film showed the approximation of the RA disc by pushing the cable while the LA disc was in the orifice of the right upper PV (A). Schematic diagram of the PV method (B). Modified balloon-assisted method and schematic diagram. Angiographic film showed both wings of the device were deployed before implantation by supporting the peripheral balloon (C). Schematic diagram of BA method (D). RA: right atrium, LA disc of the device was prevented from prolapsed into the RA by balloon (arrow head). LA: left atrium, PV: pulmonary vein, BA: balloon assisted.

Fig. 3 Flow chart of the strategy with treating ASD patients. All the patients started with the conventional method and then the modified methods were used; the BA method was the last approach after the PV method failed. If all three methods failed, surgical closure was indicated. ASD: secundum atrial septal defect, BA: balloon assisted; PV: pulmonary vein.
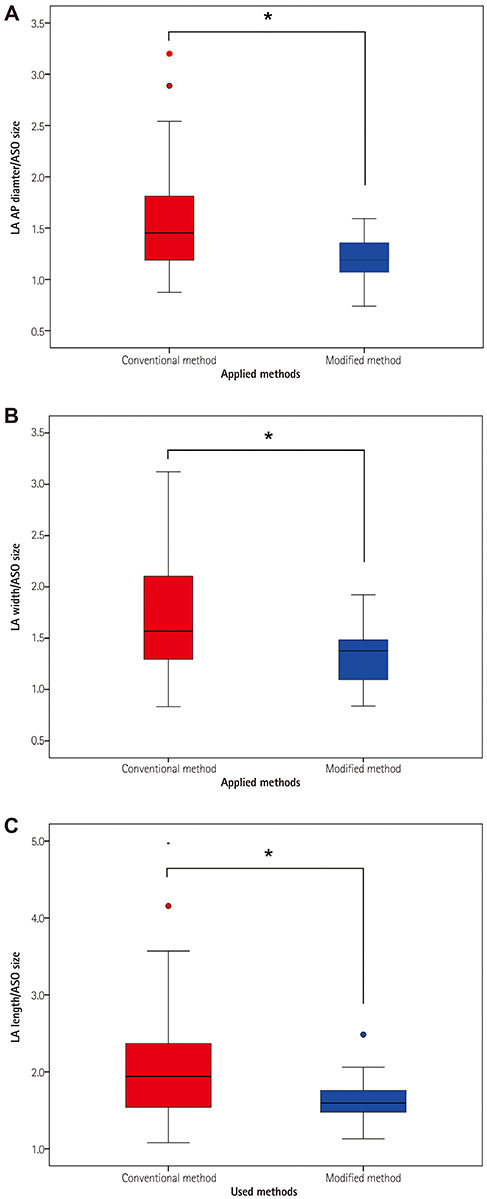
Fig. 4 Comparisons of the two groups in the ratios of the LA diameters (AP, width, and length) to the ASO size. A: ratio of LA AP diameter to ASO size. B: ratio of LA width to ASO size. C: ratio of LA length to ASO size. Pink box represented conventional group and blue box represented modified group. *Significant with p=0.001. LA: left atrium, AP: anteroposterior, ASO: Amplatzer septal occluder.

Fig. 5 ROC curve for the ratios of the LA AP diameter (red), LA width (blue), and LA length (yellow) to the ASO size. Areas under the curve were 0.719 (p=0.004), 0.716 (p=0.04), and 0.716 (p=0.004), respectively. ROC: receiveroperating characteristic, LA: left atrium, AP: anteroposterior, ASO: Amplatzer septal occluder, W: width, L: length

Fig. 6 Comparisons between the failed and successful cases in the modified methods group. A: ratio of LA AP diameter to ASO size. B: ratio of LA width to ASO size. C: ratio of LA length to ASO size. Black circle represented each of the failed cases and the blue circle represented each of the successful cases in the ratios of the LA diameters (AP, W and L) to the ASO size. LA: left atrium, AP: anteroposterior, ASO: Amplatzer septal occluder, W: width, L: length
Reference
-
1. Rosas M, Zabal C, Garcia-Montes J, Buendia A, Webb G, Attie F. Transcatheter versus surgical closure of secundum atrial septal defect in adults: impact of age at intervention. A concurrent matched comparative study. Congenit Heart Dis. 2007; 2:148–155.2. Du ZD, Hijazi ZM, Kleinman CS, Silverman NH, Larntz K. Amplatzer Investigators. Comparison between transcatheter and surgical closure of secundum atrial septal defect in children and adults: results of a multicenter nonrandomized trial. J Am Coll Cardiol. 2002; 39:1836–1844.3. Dalvi BV, Pinto RJ, Gupta A. New technique for device closure of large atrial septal defects. Catheter Cardiovasc Interv. 2005; 64:102–107.4. Papa M, Gaspardone A, Fragasso G, et al. Feasibility and safety of transcatheter closure of atrial septal defects with deficient posterior rim. Catheter Cardiovasc Interv. 2013; 81:1180–1187.5. Du ZD, Koenig P, Cao QL, Waight D, Heitschmidt M, Hijazi ZM. Comparison of transcatheter closure of secundum atrial septal defect using the Amplatzer septal occluder associated with deficient versus sufficient rims. Am J Cardiol. 2002; 90:865–869.6. Kammache I, Mancini J, Ovaert C, Habib G, Fraisse A. Feasibility of transcatheter closure in unselected patients with secundum atrial septal defect, using Amplatzer devices and a modified sizing balloon technique. Catheter Cardiovasc Interv. 2011; 78:665–674.7. Wahab HA, Almossawy A, Al Bitar I, Hijazi ZM. Tips and tricks to prevent prolapse of the Amplatzer septal occluder through large atrial septal defects. Catheter Cardiovasc Interv. 2011; 78:1041–1044.8. Huang CF, Fang CY, Ko SF, et al. Transcatheter closure of atrial septal defects with superior-anterior rim deficiency using Amplatzer septal occluder. J Formos Med Assoc. 2007; 106:986–991.9. Butera G, Romagnoli E, Carminati M, et al. Treatment of isolated secundum atrial septal defects: impact of age and defect morphology in 1,013 consecutive patients. Am Heart J. 2008; 156:706–712.10. Park SJ, Kim NK, Kim JO, Yoo BW, Choi JY, Sul JH. Morphologic characteristics and relating factors to the need of technical modification in transcatheter closure of large atrial septal defect (>/=25 mm). Korean Circ J. 2010; 40:191–196.11. Hijazi ZM. Device closure of secundum atrial septal defects: to balloon size or not to balloon size. Ann Pediatr Cardiol. 2011; 4:34–35.12. Carlson KM, Justino H, O'Brien RE. Transcatheter atrial septal defect closure: modified balloon sizing technique to avoid overstretching the defect and oversizing the Amplatzer septal occluder. Catheter Cardiovasc Interv. 2005; 66:390–396.13. Rigatelli G, Dell'avvocata F, Cardaioli P, et al. Safety and long-term outcome of modified intracardiac echocardiography-assisted "noballoon" sizing technique for transcatheter closure of ostium secundum atrial septal defect. J Interv Cardiol. 2012; 25:628–634.14. Wiley JM, White CJ, Uretsky BF. Noncoronary complications of coronary intervention. Catheter Cardiovasc Interv. 2002; 57:257–265.15. Chessa M, Carminati M, Butera G, et al. Early and late complications associated with transcatheter occlusion of secundum atrial septal defect. J Am Coll Cardiol. 2002; 39:1061–1065.16. Abaci A, Unlu S, Alsancak Y, Kaya U, Sezenoz B. Short and long term complications of device closure of atrial septal defect and patent foramen ovale: meta-analysis of 28,142 patients from 203 studies. Catheter Cardiovasc Interv. 2013; 82:1123–1138.17. Crawford GB, Brindis RG, Krucoff MW, Mansalis BP, Carroll JD. Percutaneous atrial septal occluder devices and cardiac erosion: a review of the literature. Catheter Cardiovasc Interv. 2012; 80:157–167.18. Raghuram AR, Krishnan R, Kumar S, Balamurugan K. Complications in atrial septal defect device closure. Interact Cardiovasc Thorac Surg. 2008; 7:167–169.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum to: Small Left Atrial Size Complicating Percutaneous Transcatheter Device Closure of Secundum Atrial Septal Defect with Conventional Approach
- Emergent Surgical Intervention for Embolization of Atrial Septal Defect Closure Device
- The Operative Management of Embolized Septal Occluder at Ascending Aorta
- Transcatheter Closure of Secundum Atrial Septal Defect with the Amplatzer Septal Occluder
- Estimation of Size of Adult Atrial Septal Defect
