Short-term Clinical Outcomes of Implantable Collamer Lens Implantation with Simultaneous Full Thickness Astigmatic Keratotomy
- Affiliations
-
- 1Onnuri Smile Eye Clinic, Seoul, Korea. ytchungc@daum.net
- KMID: 2388179
- DOI: http://doi.org/10.3341/jkos.2017.58.8.916
Abstract
- PURPOSE
To evaluate the clinical outcomes of implantable collamer lens (ICL) implantation with simultaneous full thickness astigmatic keratotomy (FTAK) for the correction of moderate to high myopic astigmatism.
METHODS
Thirty-two eyes of 16 patients who had an ICL implantation with simultaneous FTAK were studied. Follow-up visits were at 1 week, 1 month, and 3 months. The outcome measures included the uncorrected distance visual acuity (UDVA), refractive error, efficacy, safety, and predictability.
RESULTS
After the surgery, astigmatism was reduced by 74.83 ± 13.8%. The proportion of eyes with a spherical equivalent of 0.5 D or less was 87.5%, and all eyes had a spherical equivalent of 1.0 D or less at 3 months after the surgery. The proportion of eyes with a UDVA of 20/25 or better was 100%, and 20/20 or better was 81.25%. Reoperation was needed in one case (3.1%) because of undercorrection of the astigmatism, and no complications were observed.
CONCLUSIONS
This study showed that ICL implantation with simultaneous FTAK is effective and safe for the correction of moderate to high myopic astigmatism.
Keyword
MeSH Terms
Figure
-

Figure 1. Implantable collamer lens implantation with full thickness astigmatic keratotomy. (A) Corneal marking at the steepest axis with marking pen using CALLISTO eye® system (Carl Zeiss Meditec AG, Jena, Germany). (B) Ring marking using a ring marker with cross wires (7.5 mm). (C) Beveled, full thickness corneal incision at the steepest axis with a 2.8 mm blade. (D) Implantable collamer lens implantation through the incision. (E) Extension of the cor-neal incision with a wider blade.
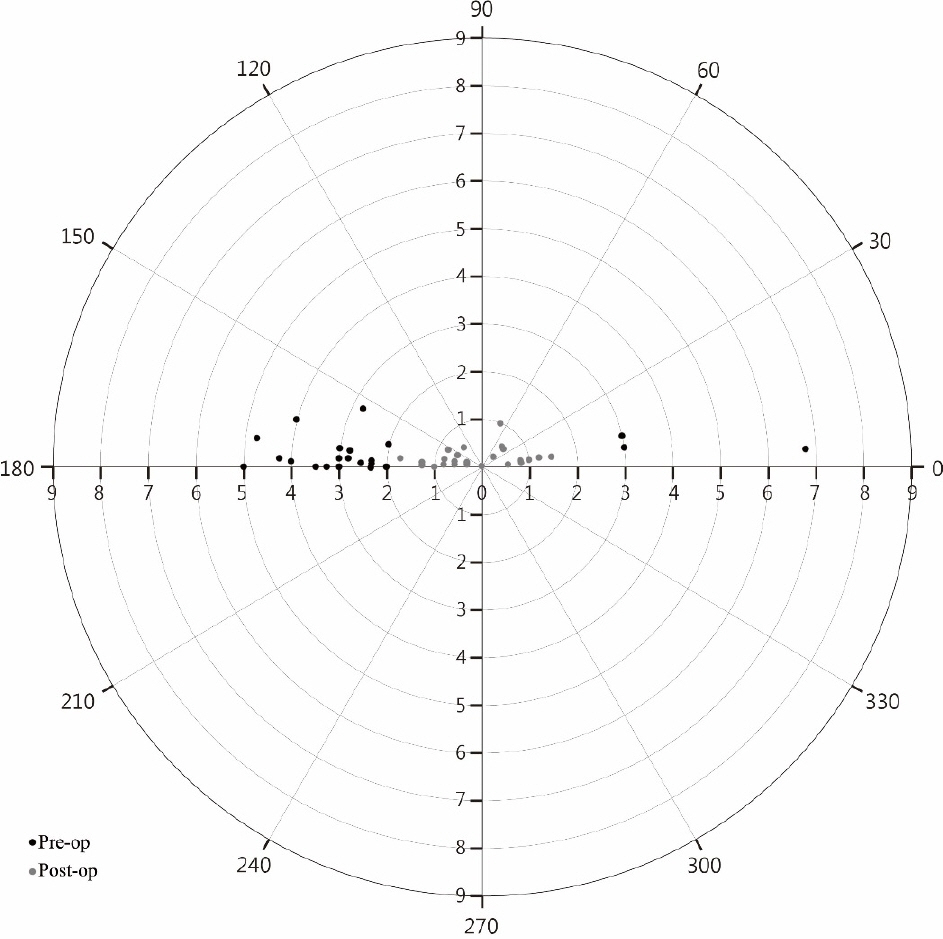
Figure 2. Vector analysis of astigmatism. This polar plot shows the reduction in astigmatism after implantable collamer lens im-plantation with simultaneous astigmatic keratotomy. Gray dots (postoperative) are closer to the center compared to black dots (preoperative). Pre-op = preoperation; Post-op = postoperation.
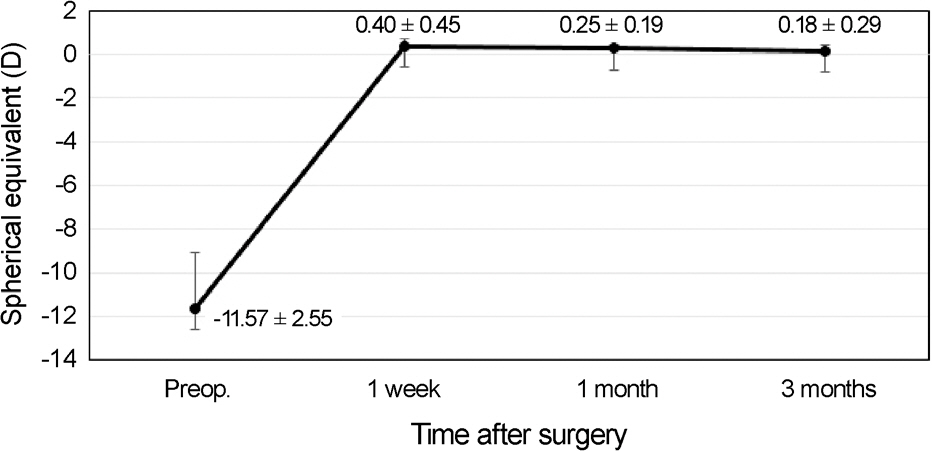
Figure 3. Stability of the implantable collamer lens im-plantation with simultaneous astigmatic keratotomy. Spherical equivalent refraction of combined procedure is stable for 3 months. Preop = preoperation.
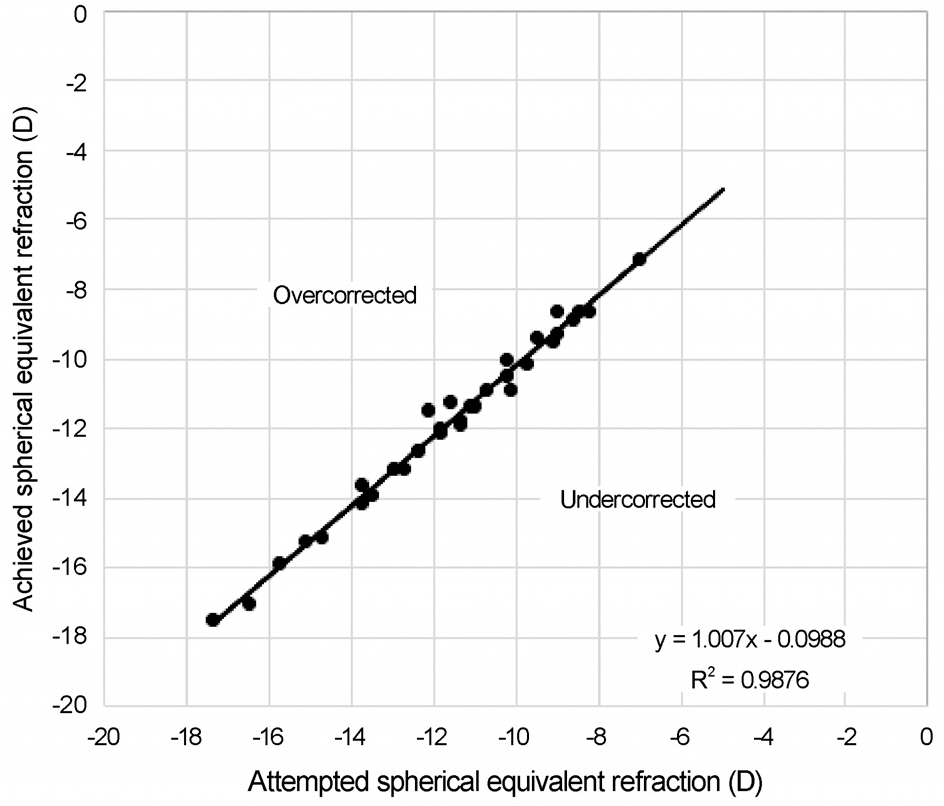
Figure 4. Predictability of the implantable collamer lens im-plantation with simultaneous astigmatic keratotomy. Scatterplot of the attempted spherical equivalent refractive change plotted against the achieved spherical equivalent change at 3 months.

Figure 5. Safety of the implantable collamer lens implantation with simultaneous astigmatic keratotomy. The percentage of eyes in which there was a gain/loss of Snellen visual acuity lines (CDVA). CDVA = corrected distance visual acuity.
Reference
-
References
1. Kamiya K, Shimizu K, Igarashi A. . Four-year follow-up of posterior chamber phakic intraocular lens implantation for moder-ate to high myopia. Arch Ophthalmol. 2009; 127:845–50.
Article2. Alfonso JF, Baamonde B, Fernández-Vega L. . Posterior cham-ber collagen copolymer phakic intraocular lenses to correct my-opia: five-year follow-up. J Cataract Refract Surg. 2011; 37:873–80.
Article3. Igarashi A, Shimizu K, Kamiya K. Eight-year follow-up of posteri-or chamber phakic intraocular lens implantation for moderate to high myopia. Am J Ophthalmol. 2014; 157:532–9.e1.
Article4. Zaldivar R, Davidorf JM, Oscherow S. Posterior chamber phakic intraocular lens for myopia of-8 to- 19 diopters. J Refract Surg. 1998; 14:294–305.5. Alfonso JF, Palacios A, Montés-Micó R. Myopic phakic STAAR collamer posterior chamber intraocular lenses for keratoconus. J Refract Surg. 2008; 24:867–74.
Article6. Kamiya K, Shimizu K, Aizawa D. . One-year follow-up of pos-terior chamber toric phakic intraocular lens implantation for mod-erate to high myopic astigmatism. Ophthalmology. 2010; 117:2287–94.
Article7. Kamiya K, Shimizu K, Kobashi H. . Three-year follow-up of posterior chamber toric phakic intraocular lens implantation for moderate to high myopic astigmatism. PLoS One. 2013; 8:e56453.
Article8. Yoon JM, Moon SJ, Lee KH. Clinical outcomes of toric implant-able collamer lens implantation. J Korean Ophthalmol Soc. 2009; 50:839–51.
Article9. Kim BK, Mun SJ, Lee DG, Chung YT. Clinical outcomes of com-bined procedure of astigmatic keratotomy and laser in situ keratomileusis. J Korean Ophthalmol Soc. 2016; 57:353–60.10. Kim BK, Mun SJ, Lee DG. . Full-thickness astigmatic keratot-omy combined with small-incision lenticule extraction to treat high-level and mixed astigmatism. Cornea. 2015; 34:1582–7.
Article11. Kim BK, Mun SJ, Lee DG, Chung YT. Clinical outcomes of bev-eled, full thickness astigmatic keratotomy. J Korean Ophthalmol Soc. 2015; 56:1160–9.
Article12. Tatar MG, Aylin Kantarci F, Yildirim A. . Risk factors in post-LASIK corneal ectasia. J Ophthalmol. 2014; 2014:204191.
Article13. Ivarsen A, Næser K, Hjortdal J. Laser in situ keratomileusis for high astigmatism in myopic and hyperopic eyes. J Cataract Refract Surg. 2013; 39:74–80.
Article14. Bhandari V, Karandikar S, Reddy JK, Relekar K. Implantable col-lamer lens V4b and V4c for correction of high myopia. J Curr Ophthalmol. 2016; 27:76–81.
Article15. Park SC, Kwun YK, Chung ES. . Postoperative astigmatism and axis stability after implantation of the STAAR toric implant-able collamer lens. J Refract Surg. 2009; 25:403–9.
Article16. Mori T, Yokoyama S, Kojima T. . Factors affecting rotation of a posterior chamber collagen copolymer toric phakic intraocular lens. J Cataract Refract Surg. 2012; 38:568–73.
Article17. Gomez-Bastar A, Jaimes M, Graue-Hernández EO. . Long- term refractive outcomes of posterior chamber phakic (spheric and toric implantable collamer lens) intraocular lens implantation. Int Ophthalmol. 2014; 34:583–90.18. Kamiya K, Shimizu K, Aizawa D. . Surgically induced astig-matism after posterior chamber phakic intraocular lens implantation. Br J Ophthalmol. 2009; 93:1648–51.
Article19. Pineda R, Jain V. Arcuate keratotomy: an option for astigmatism correction after laser in situ keratomileusis. Cornea. 2009; 28:1178–80.
Article20. Song HB, Choi HJ, Kim MK, Wee WR. The short-term effect of limbal relaxing incision and compression suture on post-penetrating keratoplasty astigmatism. J Korean Ophthalmol Soc. 2011; 52:1142–9.
Article21. Nubile M, Carpineto P, Lanzini M. . Femtosecond laser arcuate keratotomy for the correction of high astigmatism after keratoplasty. Ophthalmology. 2009; 116:1083–92.
Article22. Hoffart L, Proust H, Matonti F. . Correction of postkeratoplasty astigmatism by femtosecond laser compared with mechanized as-tigmatic keratotomy. Am J Ophthalmol. 2009; 147:779–87.e1.
Article23. Buzzonetti L, Petrocelli G, Laborante A. . Arcuate keratotomy for high postoperative keratoplasty astigmatism performed with the intralase femtosecond laser. J Refract Surg. 2009; 25:709–14.
Article24. Kumar NL, Kaiserman I, Shehadeh-Mashor R. . IntraLase-en-abled astigmatic keratotomy for post-keratoplasty astigmatism: on-axis vector analysis. Ophthalmology. 2010; 117:1228–35.e1.
Article25. Mendicute J, Irigoyen C, Ruiz M. . Toric intraocular lens ver-sus opposite clear corneal incisions to correct astigmatism in eyes having cataract surgery. J Cataract Refract Surg. 2009; 35:451–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Outcomes of Beveled, Full Thickness Astigmatic Keratotomy
- Long-term Clinical Outcomes of Implantable Collamer Lens
- Axial Length Change after Implantable Collamer Lens Implantation
- Partial Visual Rehabilitation Using a Toric Implantable Collamer Lens in a Patient with Keratoconus: A Case Report with 20 Months of Follow-up
- Clinical Outcomes of Combined Procedure of Astigmatic Keratotomy and Laser in situ Keratomileusis
