Conservative Treatment for Juvenile Osteochondritis Dissecans of the Talus
- Affiliations
-
- 1Department of Orthopaedic Surgery, Pusan National University Hospital, Busan, Korea. kimht@pusan.ac.kr
- 2Department of Orthopaedic Surgery, Inje University Haeundae Paik Hospital, Busan, Korea.
- KMID: 2387789
- DOI: http://doi.org/10.4055/jkoa.2017.52.4.310
Abstract
- PURPOSE
We compared the results between conservative and surgical treatment methods in a group of children and adolescents with osteochondritis dissecans of the talus.
MATERIALS AND METHODS
A total of 24 patients (31 ankles), who were younger than 18 years old, were included in this study. Group 1 consisted of 14 ankles (mean age at the time of treatment was 13.0 years) treated conservatively. Group 2 consisted 17 ankles (mean age at the time of treatment was 15.1 years) treated surgically. According to the Berndt and Harty classification, there were 6 ankles in class I, 4 in class II, 3 in class III, and 1 in class IV in group 1; 1 ankle in class I, 9 in class II, and 7 in class III in group 2. In group 1, there were 13 medial lesions and 1 lateral lesion; and in group 2, there were 14 medial lesions and 3 lateral lesions. The mean follow-up period was 31.9 months for group 1 and 28.9 months for group 2. Clinical and radiologic results were analyzed using the American Orthopaedic Foot and Ankle Society (AOFAS) score and the classification by Higuera et al.
RESULTS
The mean AOFAS clinical score was 91.4 in group 1 and 87.5 in group 2. According to the classification by Higuera et al., regarding clinical results, there were 6 excellent, 7 good, and 1 fair in group 1, and 5 excellent, 2 good, and 10 fair in group 2. As for radiological results, there were 13 good and 1 fair in group 1, and 10 good and 7 fair in group 2. There was no statistical difference between the two groups.
CONCLUSION
Conservative treatment provided satisfactory results for osteochondritis dissecans of the talus in children and adolescents.
Keyword
MeSH Terms
Figure
-
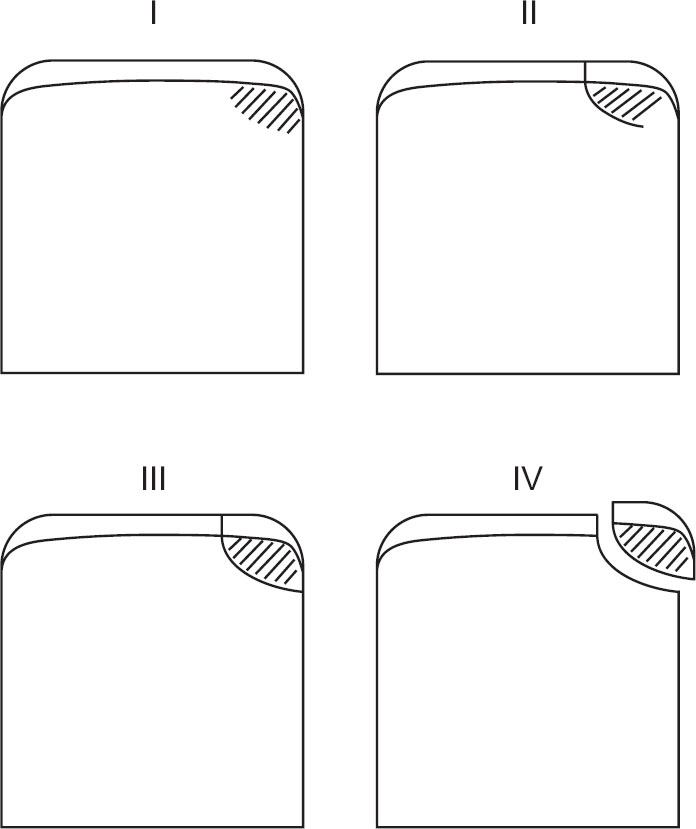
Figure 1 Schematic drawings of four stages of osteochondritis dissecans of the talus in the radiographs (classified by Berndt and Harty): Stage I is compression of the affected subchondral bone, stage II is partially attached avulsion of the transchondral bone, stage III is completely detached but not displaced, and stage IV is displaced fragment.

Figure 2 (A) Initial anteroposterior (AP) radiograph of the right ankle in a 12-year-old boy (case 3 in the group 1) showed osteochondritis dissecans of the talus located in the lateral side. He did not have any traumatic history in the affected side, but had ankle pain for several months; he was finally treated with a cast at another hospital. He was classified in accordance with the Berndt and Harty classification15) as stage II. In serial T2-weighted fat suppression coronal (B) and sagittal (C) magnetic resonance imagings (MRIs), which were taken at the time of his first visit to another hospital, the overlying chondral surface of the talus was intact and continuous with the healthy part (stage II according to the classification by Dipaola et al.16)). (B, C) The fragment was not separated from the talus contraindicating the ostechondral fracture of the talus. During the follow-up period, he experienced aggravated pain. He was then transferred to hospital and treated conservatively. (D) AP radiograph showed that the bony fragment was slightly displaced (Berndt and Harty's stage IV). A short leg cast was applied for 4 weeks and then a brace was applied for 2 months. T1-weighted coronal (E) and sagittal (F) MRIs, which were taken 4 months after conservative treatment (9 months after initial diagnosis at another hospital), showed an enlarged lesion, but with decreased pain (stage II according to the classification by Dipaloa et al.16)). (G) The last follow-up radiograph of the right ankle taken 4 years after the initial treatment showed a decreased gap in the lesion. His clinical result (by Higuera et al.18)) was good.

Figure 3 (A) Initial anteroposterior radiograph of the right ankle in an 11-year-old boy (case 1 in the group 1) showed osteochondritis dissecans of the talus located in the medial side. He was classified as stage III in accordance with the Berndt and Harty classification.15) He had a similar lesion in the left ankle. A short leg cast was applied for 4 weeks and subsequently a brace for 2 months. T1 weighted coronal (B) and sagittal (C) magnetic resonance imagings, which were taken four years and seven months later, showed remaining lesions (stage II according to the classification by Dipaola et al.16)). (D) The last follow-up radiograph of the right ankle, which was taken five years and six months after the initial visit, showed the lesion healing. His clinical result (classification by Higuera et al.18)) was excellent; he had mild symptoms in the right ankle during running.
Cited by 2 articles
-
Natural History of Osteochondral Lesion of the Talus
Min Gyu Kyung, Dong-Oh Lee, Dong Yeon Lee
J Korean Foot Ankle Soc. 2020;24(2):37-41. doi: 10.14193/jkfas.2020.24.2.37.Osteochondral Lesion of the Talus in Children and Adolescents
Mi Hyun Song
J Korean Orthop Assoc. 2018;53(3):210-217. doi: 10.4055/jkoa.2018.53.3.210.
Reference
-
1. Aichroth P. Osteochondritis dissecans of the knee. A clinical survey. J Bone Joint Surg Br. 1971; 53:440–7.2. Aichroth P. Osteochondral fractures and their relationship to osteochondritis dissecans of the knee. An experimental study in animals. J Bone Joint Surg Am. 1971; 53:448–54.3. Hefti F, Beguiristain J, Krauspe R. . Osteochondritis dissecans: a multicenter study of the European Pediatric Orthopedic Society. J Pediatr Orthop B. 1999; 8:231–45.4. O'Farrell TA, Costello BG. Osteochondritis dissecans of the talus. The late results of surgical treatment. J Bone Joint Surg Br. 1982; 64:494–7.5. Van DeMark RE. Osteochondritis dissecans with spontaneous healing. J Bone Joint Surg Am. 1952; 35:143–8.
Article6. Smillie IS. Treatment of osteochondritis dissecans. J Bone Joint Surg Br. 1957; 39:248–60.
Article7. Lahm A, Erggelet C, Steinwachs M, Reichelt A. Arthroscopic management of osteochondral lesions of the talus: results of drilling and usefulness of magnetic resonance imaging before and after treatment. Arthroscopy. 2000; 16:299–304.
Article8. Lam KY, Siow HM. Conservative treatment for juvenile osteochondritis dissecans of the talus. J Orthop Surg (Hong Kong). 2012; 20:176–80.
Article9. McCullough CJ, Venugopal V. Osteochondritis dissecans of the talus: the natural history. Clin Orthop Relat Res. 1979; 144:264–8.10. Anderson DV, Lyne ED. Osteochondritis dissecans of the talus: case report on two family members. J Pediatr Orthop. 1984; 4:356–7.11. Gepstein R, Conforty B, Weiss RE, Hallel T. Closed percutaneous drilling for osteochondritis dissecans of the talus. A report of two cases. Clin Orthop Relat Res. 1986; 213:197–200.12. Bruns J, Rosenbach B. Osteochondrosis dissecans of the talus. Comparison of results of surgical treatment in adolescents and adults. Arch Orthop Trauma Surg. 1992; 112:23–7.13. Kumai T, Takakura Y, Higashiyama I, Tamai S. Arthroscopic drilling for the treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 1999; 81:1229–35.
Article14. Gautier E, Kolker D, Jakob RP. Treatment of cartilage defects of the talus by autologous osteochondral grafts. J Bone Joint Surg Br. 2002; 84:237–44.
Article15. Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959; 41:988–1020.
Article16. Dipaola JD, Nelson DW, Colville MR. Characterizing osteochondral lesions by magnetic resonance imaging. Arthros-copy. 1991; 7:101–4.
Article17. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myer-son MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994; 15:349–53.
Article18. Higuera J, Laguna R, Peral M, Aranda E, Soleto J. Osteochondritis dissecans of the talus during childhood and adolescence. J Pediatr Orthop. 1998; 18:328–32.
Article19. Kessler JI, Weiss JM, Nikizad H. . Osteochondritis dissecans of the ankle in children and adolescents: demographics and epidemiology. Am J Sports Med. 2014; 42:2165–71.20. Roden WM, Tillegard P, Unanderscharin L. Osteochondritis dissecans and similar lesions of the talus: report of fifty-five cases with special reference to etiology and treatment. Acta Orthop Scand. 1953; 23:51–66.21. Letts M, Davidson D, Ahmer A. Osteochondritis dissecans of the talus in children. J Pediatr Orthop. 2003; 23:617–25.
Article22. Canale ST, Belding RH. Osteochondral lesion of the talus. J Bone Joint Surg Am. 1980; 62:97–102.23. Trinh TQ, Harris JD, Flanigan DC. Surgical management of juvenile osteochondritis dissecans of the knee. Knee Surg Sports Traumatol Arthrosc. 2012; 20:2419–29.
Article24. Jürgensen I, Bachmann G, Schleicher I, Haas H. Arthroscop-ic versus conservative treatment of osteochondritis dissecans of the knee: value of magnetic resonance imaging in therapy planning and follow-up. Arthroscopy. 2002; 18:378–86.25. Kijowski R, Blankenbaker DG, Shinki K, Fine JP, Graf BK, De Smet AA. Juvenile versus adult osteochondritis dissecans of the knee: appropriate MR imaging criteria for instability. Radiology. 2008; 248:571–8.
Article26. Stone JW. Osteochondral lesions of the talar dome. J Am Acad Orthop Surg. 1996; 4:63–73.
Article27. Ferkel RD, Whipple TL. Arthroscopic surgery: the foot and ankle. Philadelphia: Lippincott Raven;. 1996.28. Pritsch M, Horoshovski H, Farine I. Arthroscopic treatment of osteochondral lesions of the talus. J Bone Joint Surg Am. 1986; 68:862–5.
Article29. Roßbach BP, Paulus AC, Niethammer TR, et al. Discrepancy between morphological findings in juvenile osteochondritis dissecans (OCD): a comparison of magnetic resonance imaging (MRI) and arthroscopy. Knee Surg Sports Traumatol Arthrosc. 2016; 24:1259–64.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Osteochondritis Dissecans of Talus
- Outcomes of Operative Management of Juvenile Osteochondritis Dissecans of the Knee in Athletes
- Osteochondritis Dissecans of the Knee Associated with Gout: A Case Report
- Osteochondritis Dissecans of the Capitellum Humeri: Analysis of C. T. Findings
- Osteochondritis Dissecans of Femoral Head Following Legg-Calve-Perthes Disease
