Full mouth rehabilitation in a patient with partial mandibulectomy using CAD/CAM zirconia framework and monolithic zirconia
- Affiliations
-
- 1Department of Prosthodontics, School of Dentistry, Chonnam National University, Gwangju, Republic of Korea. mcnihil@jnu.ac.kr
- 2Department of Oral and Maxillofacial Surgery, School of Dentistry, Chonnam National University, Gwangju, Republic of Korea.
- 3Department of Oral Medicines, School of Dentistry, Chonnam National University, Gwangju, Republic of Korea.
- 4Design Dental Clinic, Gwangju, Republic of Korea.
- KMID: 2387200
- DOI: http://doi.org/10.4047/jkap.2017.55.3.279
Abstract
- Defects due to mandibulectomy often cause hard and soft tissue loss and result in esthetic problems and functional disorders such as mastication, swallowing, and pronunciation. After the mandibular reconstruction, several complications including loss of alveolar bone can cause limitations in maintenance or supporting of removable prosthesis. For these patients, implant-supported fixed restorations have been an appropriate prosthetic restorative method. In this case report, we report the patient who underwent mandibulectomy and mandibular reconstruction owing to oral cancer, and then restored the current dentition functionally and aesthetically by applying zirconia frameworks and monolithic zirconia crowns by computer-aided design and computer-aided manufacturing.
Keyword
MeSH Terms
Figure
-

Fig. 1. Pretreatment condition. (A) Frontal view, (B) radiograph after mandibulectomy, (C) radiograph after surgical reconstruction.
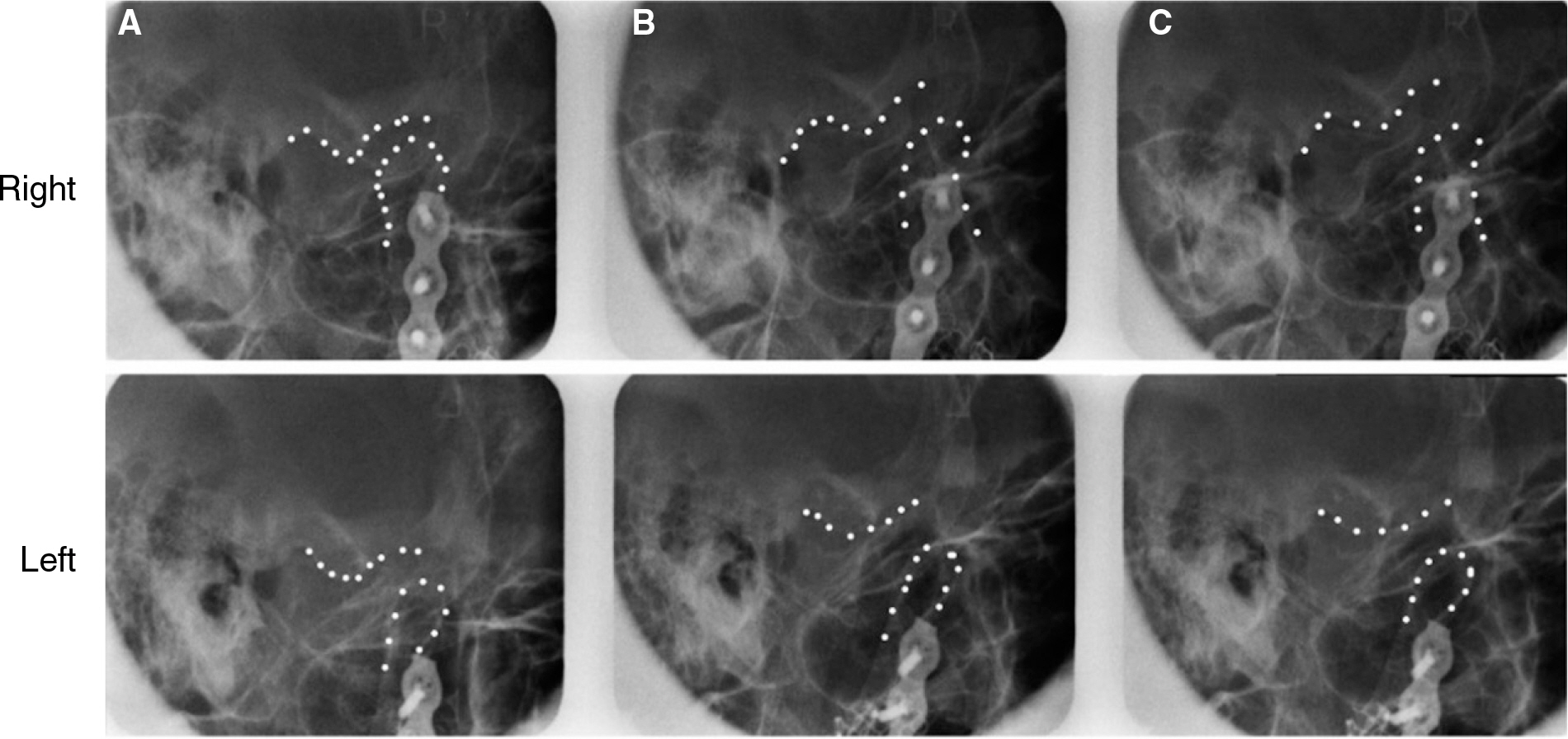
Fig. 2. Transcranial radiograph. Right and left TMJ at closing (A), 1 inch opening (B) and maximum opening (C).

Fig. 3. Panoramic radiograph after implant surgery.

Fig. 4. A screw-retained interim prosthesis with temporary abutments and autopolymerizing acrylic resin. (A) Frontal view, (B, C) Occlusal intraoral photo.

Fig. 5. Computer-aided design of customized titanium abutments (A) and monolithic zirconia framework (B).

Fig. 6. (A) Monolithic zirconia framework and interim restorations, (B) Intraoral placement.

Fig. 7. Plaque deposition below the framework.
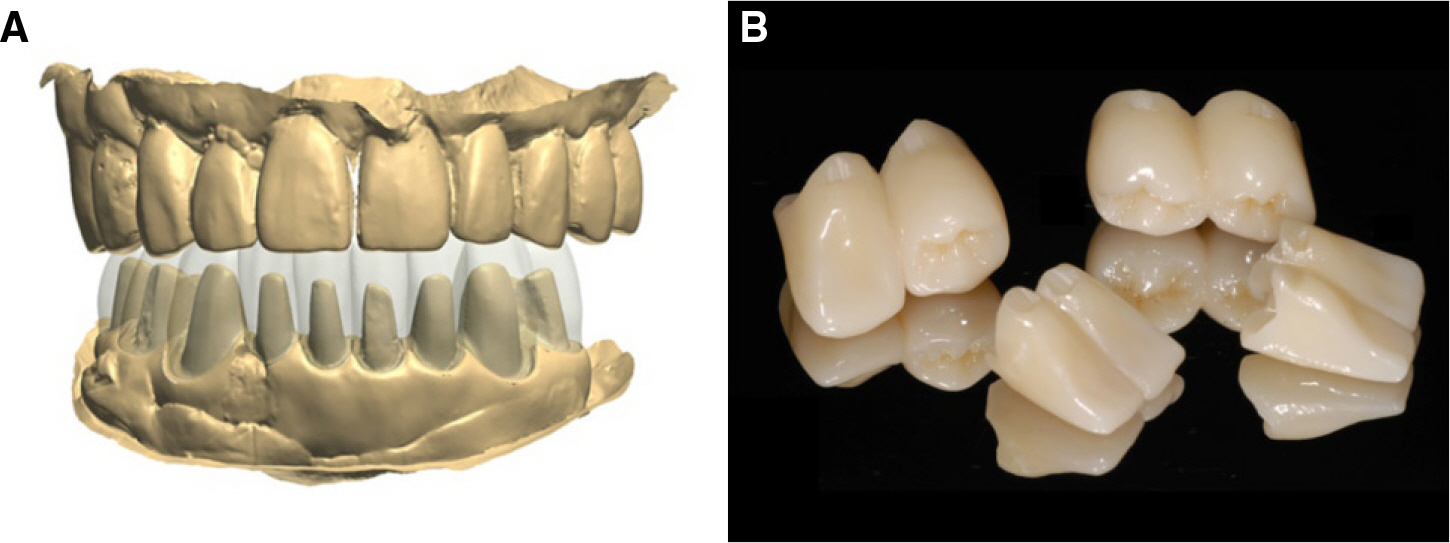
Fig. 8. (A) Superimposition of interim restorations and framework. (B) Anatomic contour zirconia crowns with notch.
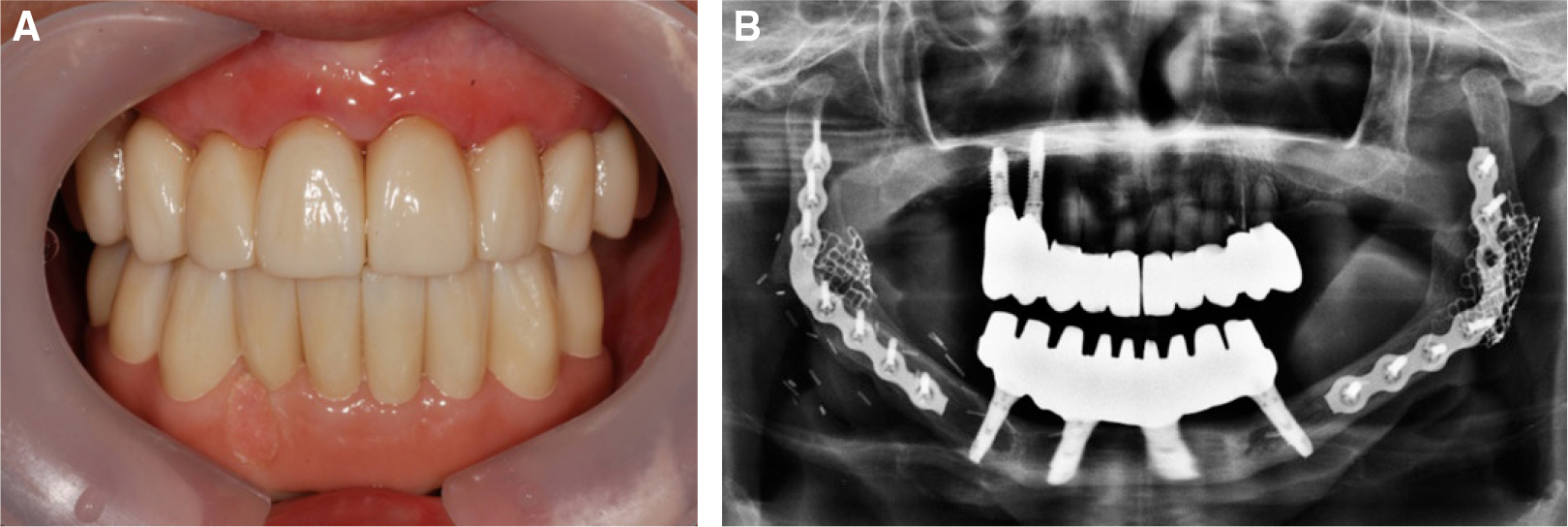
Fig. 9. Definitive dental prosthesis after placement. (A) Intraoral photo, (B) Panoramic radiograph.
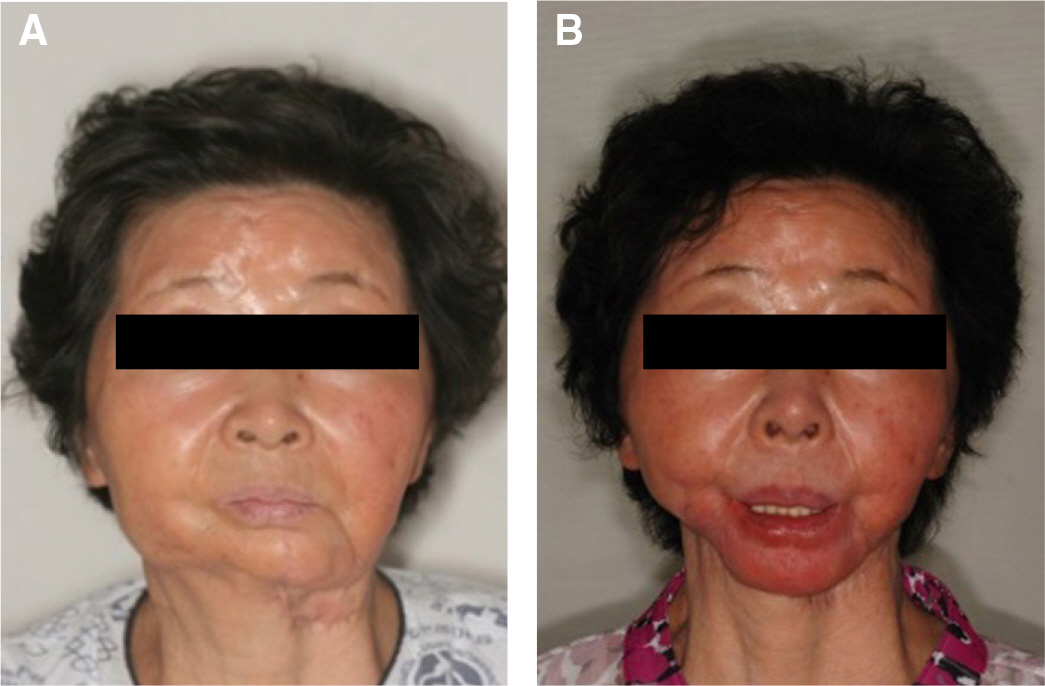
Fig. 10. Patient's profile. (A) Profile at first visit, (B) Profile after definitive prosthesis placement.
Reference
-
1.Tjellstrom A., Jansson K., Brånemark PI. Craniofacial defects. Worthington P, Brånemark PI, Stream C, editors. Advanced os-seointegration surgery. Chicago: Quintessence;1992. p. 293–312.2.Landes CA. Zygoma implant-supported midfacial prosthetic rehabilitation: a 4-year follow-up study including assessment of quality of life. Clin Oral Implants Res. 2005. 16:313–25.
Article3.Drago C., Gurney L. Maintenance of implant hybrid prostheses: clinical and laboratory procedures. J Prosthodont. 2013. 22:28–35.
Article4.Sadowsky SJ. The implant-supported prosthesis for the edentulous arch: design considerations. J Prosthet Dent. 1997. 78:28–33.
Article5.Jemt T., Johansson J. Implant treatment in the edentulous maxillae: a 15-year follow-up study on 76 consecutive patients provided with fixed prostheses. Clin Implant Dent Relat Res. 2006. 8:61–9.
Article6.Jemt T. Fixed implant-supported prostheses in the edentulous maxilla. A five-year follow-up report. Clin Oral Implants Res. 1994. 5:142–7.
Article7.Drago C., Howell K. Concepts for designing and fabricating metal implant frameworks for hybrid implant prostheses. J Prosthodont. 2012. 21:413–24.
Article8.Chronopoulos V., Kourtis S., Katsikeris N., Nagy W. Tooth- and tissue-supported provisional restorations for the treatment of patients with extended edentulous spans. J Esthet Restor Dent. 2009. 21:7–17.9.Jemt T., Lekholm U. Measurements of bone and framework deformations induced by misfit of implant superstructures. A pilot study in rabbits. Clin Oral Implants Res. 1998. 9:272–80.
Article10.Jemt T., Lie A. Accuracy of implant-supported prostheses in the edentulous jaw: analysis of precision of fit between cast gold-alloy frameworks and master casts by means of a three-dimensional photogrammetric technique. Clin Oral Implants Res. 1995. 6:172–80.
Article11.Drago C., Saldarriaga RL., Domagala D., Almasri R. Volumetric determination of the amount of misfit in CAD/CAM and cast implant frameworks: a multicenter laboratory study. Int J Oral Maxillofac Implants. 2010. 25:920–9.12.Piconi C., Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials. 1999. 20:1–25.
Article13.Manicone PF., Rossi Iommetti P., Raffaelli L. An overview of zirconia ceramics: basic properties and clinical applications. J Dent. 2007. 35:819–26.
Article14.Lee BC., Jung GY., Kim DJ., Han JS. Initial bacterial adhesion on resin, titanium and zirconia in vitro. J Adv Prosthodont. 2011. 3:81–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation using monolithic zirconia: a clinical report
- Full mouth rehabilitation of a patient using monolithic zirconia and dental CAD/CAM system: a case report
- Maxillary cement retained implant supported monolithic zirconia prosthesis in a full mouth rehabilitation: a clinical report
- Esthetic anterior restoration using 3M Lavaâ„¢ Esthetic monolithic zirconia
- Full mouth rehabilitation with vertical dimension increase in patient with severly worn dentition
