Intractable Atrial Flutter Successfully Treated with Flecainide and Propranolol in a Premature Infant
- Affiliations
-
- 1Department of Pediatrics, Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea.
- 2Department of Pediatrics, Ewha Womans University School of Medicine, Seoul, Korea. jeban@naver.com
- KMID: 2386392
- DOI: http://doi.org/10.12771/emj.2017.40.3.140
Abstract
- Although Atrial flutter (AFL) in newborn infant with normal cardiac anatomy has benign clinical course, an intractable AFL is associated with an increased risk of development of heart failure and sudden death, and is still difficult to manage. It requires multiple external electrical cardioversions, and it shows a poor response to antiarrhythmic drug therapy. We report a case of a premature infant with an intractable AFL, which we successfully treated with oral flecainide and propranolol in spite of recurred AFL. A 1-month-old, 34-week gestation, premature baby presented with an irregular heart beat and irritability. An AFL with 2:1 atrioventricular conduction was documented. Because of the intractable AFL, repeated electrical cardioversion and amiodarone were continued for 14 days. However, amiodarone was discontinued in favour of flecainide and propranolol because of the recurrent AFL and newly developed transient hypothyroidism. During 1-year follow-up period, in which oral flecainide and propranolol were continued, no AFL was observed.
Keyword
MeSH Terms
Figure
-
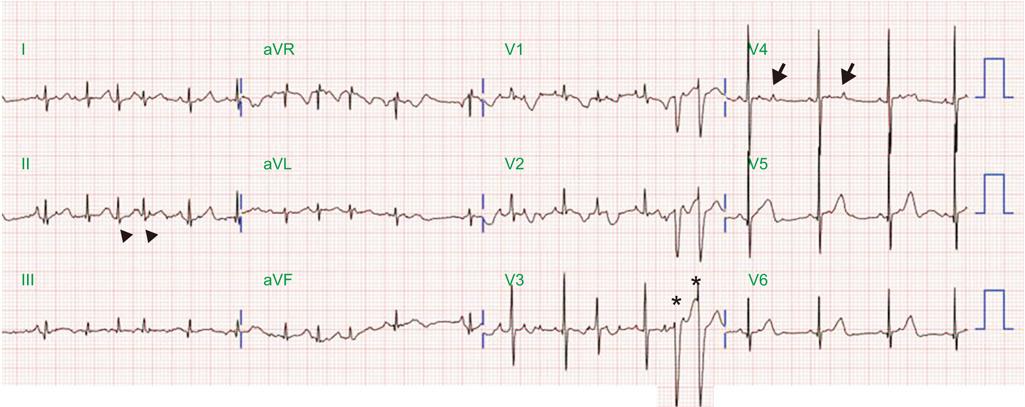
Fig. 1 A baseline 12-lead surface electrocardiogram. Premature atrial complexes (arrowhead) with non-conduction (arrow) and aberrant conduction (asterisk) are shown. aVR, augmented vector right; aVL, augmented vector left; aVF, augmented vector foot.

Fig. 2 Atrial flutter on an electrocardiogram. (A) A rhythm strip electrocardiogram showed narrow QRS tachycardia, with a ventricular rate of 198 beats/min. Atrial flutter with 2:1 atrioventricular conduction was documented on 12-lead electrocardiogram. (B) After the adenosine injection, a 12-lead surface electrocardiogram showed atrial flutter, with variable atrioventricular conduction and an atrial rate of 300 beats/min. AVR, augmented vector right; AVL, augmented vector left; AVF, augmented vector foot.
Reference
-
1. Dunnigan A, Benson W Jr, Benditt DG. Atrial flutter in infancy: diagnosis, clinical features, and treatment. Pediatrics. 1985; 75:725–729.
Article2. Casey FA, McCrindle BW, Hamilton RM, Gow RM. Neonatal atrial flutter: significant early morbidity and excellent long-term prognosis. Am Heart J. 1997; 133:302–306.
Article3. Texter KM, Kertesz NJ, Friedman RA, Fenrich AL Jr. Atrial flutter in infants. J Am Coll Cardiol. 2006; 48:1040–1046.
Article4. Suzumura H, Nitta A, Ono M, Arisaka O. Neonatal intractable atrial flutter successfully treated with intravenous flecainide. Pediatr Cardiol. 2004; 25:154–156.
Article5. Gulletta S, Rovelli R, Fiori R, Bella PD. Multiple external electrical cardioversions for refractory neonatal atrial flutter. Pediatr Cardiol. 2012; 33:354–356.
Article6. Knirsch W, Kretschmar O, Vogel M, Uhlemann F, Bauersfeld U. Successful treatment of atrial flutter with amiodarone in a premature neonate: case report and literature review. Adv Neonatal Care. 2007; 7:113–121.7. Obidi E, Toubas P, Sharma J. Atrial flutter in a premature infant with a structurally normal heart. J Matern Fetal Neonatal Med. 2006; 19:113–114.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of atrial flutter with fetal hydrops: successful fetal drug therapy
- Perimortem cesarean section in a pregnant woman with flecainide-induced ventricular tachycardia: A case report
- A Study on Propranolol as Anti-Arrhythmic Agent
- A case of fetal atrial flutter with hydrops fetalis
- Management of Atrial Flutter
