Comparison of Long-term Surgical Outcomes of Two-muscle Surgery in Basic-type Intermittent Exotropia: Bilateral versus Unilateral
- Affiliations
-
- 1Department of Ophthalmology, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. lsy3379@dsmc.or.kr
- 2Department of Ophthalmology, Dongguk University Gyeongju Hospital, Dongguk University College of Medicine, Gyeongju, Korea.
- KMID: 2385585
- DOI: http://doi.org/10.3341/kjo.2016.0071
Abstract
- PURPOSE
To compare long-term surgical outcomes after bilateral lateral rectus recession (BLR) and unilateral lateral rectus recession-medial rectus resection (RR) for the treatment of basic-type intermittent exotropia.
METHODS
Consecutive patients who underwent BLR or RR for treatment of intermittent exotropia between 1999 and 2010 and underwent ≥5 years of follow-up were recruited for this study. Surgical outcomes were grouped according to postoperative angle of deviation: overcorrection (esophoria/tropia >8 prism diopters [Δ]), success (esophoria/tropia ≤8Δ to exophoria/tropia ≤8Δ), and undercorrection/recurrence (exophoria/tropia >8Δ). Outcomes were compared between the BLR group and the RR group at postoperative week 1, months 1 and 6, and years 1, 2, 3, 4, and 5.
RESULTS
Of 99 patients, 37 underwent BLR and 62 underwent RR. At postoperative month 6 (97.3% vs. 82.3%, p = 0.045) and year 1 (91.9% vs. 74.2%, p = 0.040), the surgical success rates in the BLR group were significantly higher than in the RR group. Recurrence of exophoria/tropia most commonly occurred between 2 and 3 years after surgery in the BLR group, but continuous recurrences were found in the RR group. At postoperative year 5, the surgical success rate was 54.1% in the BLR group and 41.9% in the RR group (p = 0.403). The reoperation rate was 24.3% in the BLR group and 33.9% in the RR group (p = 0.317).
CONCLUSIONS
Surgical outcomes 5 years after surgery for intermittent exotropia were comparable between the BLR and RR groups. The surgical success rate and the reoperation rate were not significantly different between the BLR and RR groups.
Keyword
Figure
-
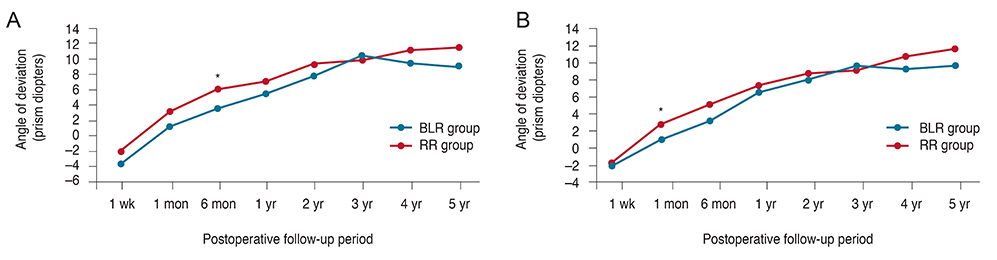
Fig. 1 Mean angles of deviation at each postoperative time point in the bilateral lateral rectus recession (BLR) group and the unilateral lateral rectus recession-medial rectus resection (RR) group treated for basic-type intermittent exotropia. (A) The mean angle of deviation at distant fixation was more exotropic in the RR group than in the BLR group through the entire follow-up period, except for postoperative year 3. (B) The mean deviation at near fixation was also more exotropic in the RR group than in the BLR group through the entire follow-up period, except postoperative year 3. *p <0.05 by independent t-test.
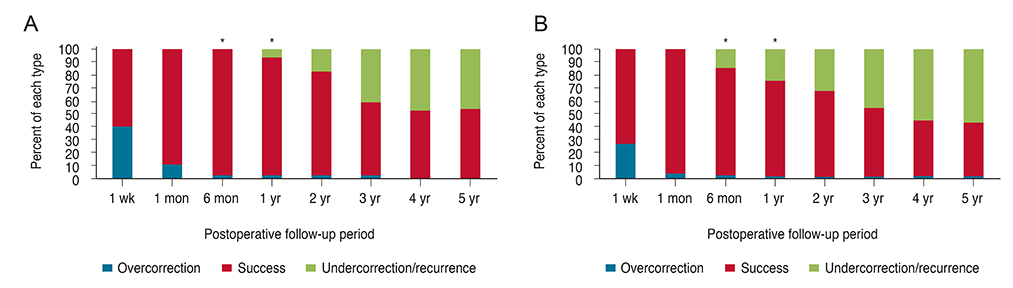
Fig. 2 The proportions of each surgical outcome type at distant fixation for each postoperative time point in the bilateral lateral rectus recession (BLR) group (A) and in the unilateral lateral rectus recession-medial rectus resection (RR) group (B) for basic-type intermittent exotropia. Surgical outcomes at postoperative month 6 (p = 0.045) and year 1 (p = 0.040) differed significantly between the groups, demonstrating a higher success rate in the BLR group than in the RR group. *p <0.05 by Pearson's chi-square test.
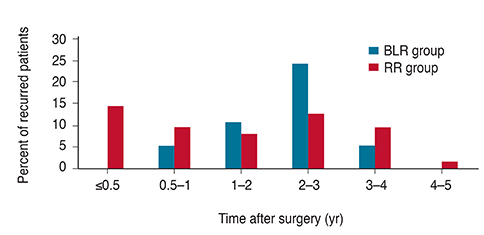
Fig. 3 The percentages of recurrence at distant fixation for each postoperative time point in the bilateral lateral rectus recession (BLR) group and the unilateral lateral rectus recession-medial rectus resection (RR) group for basic-type intermittent exotropia. Analysis showed that recurrence was most common between postoperative years 2 and 3 in the BLR group, whereas it was most common within 6 months postoperatively in the RR group with continuous recurrences after surgery.

Fig. 4 Kaplan-Meier survival analysis for recurrence of exophoria/tropia more than 8 prism diopters in the bilateral lateral rectus recession (BLR) group and the unilateral lateral rectus recession-medial rectus resection (RR) group for basic-type intermittent exotropia. The analysis showed no statistically significant difference in the cumulative probability of survival between the two groups (p = 0.531, log-rank test).
Reference
-
1. Govindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia: a population-based study. Ophthalmology. 2005; 112:104–108.2. Clarke MP. Intermittent exotropia. J Pediatr Ophthalmol Strabismus. 2007; 44:153–157.3. Gnanaraj L, Richardson SR. Interventions for intermittent distance exotropia: review. Eye (Lond). 2005; 19:617–621.4. Pineles SL, Ela-Dalman N, Zvansky AG, et al. Long-term results of the surgical management of intermittent exotropia. J AAPOS. 2010; 14:298–304.5. Pratt-Johnson JA, Barlow JM, Tillson G. Early surgery in intermittent exotropia. Am J Ophthalmol. 1977; 84:689–694.6. Hardesty HH, Boynton JR, Keenan JP. Treatment of intermittent exotropia. Arch Ophthalmol. 1978; 96:268–274.7. Richard JM, Parks MM. Intermittent exotropia: surgical results in different age groups. Ophthalmology. 1983; 90:1172–1177.8. Stoller SH, Simon JW, Lininger LL. Bilateral lateral rectus recession for exotropia: a survival analysis. J Pediatr Ophthalmol Strabismus. 1994; 31:89–92.9. Ruttum MS. Initial versus subsequent postoperative motor alignment in intermittent exotropia. J AAPOS. 1997; 1:88–91.10. Olitsky SE. Early and late postoperative alignment following unilateral lateral rectus recession for intermittent exotropia. J Pediatr Ophthalmol Strabismus. 1998; 35:146–148.11. Yam JC, Wu PK, Chong GS, et al. Long-term ocular alignment after bilateral lateral rectus recession in children with infantile and intermittent exotropia. J AAPOS. 2012; 16:274–279.12. Kushner BJ. Selective surgery for intermittent exotropia based on distance/near differences. Arch Ophthalmol. 1998; 116:324–328.13. Yuksel D, Spiritus M, Vandelannoitte S. Symmetric or asymmetric surgery for basic intermittent exotropia. Bull Soc Belge Ophtalmol. 1998; 268:195–199.14. Ing MR, Nishimura J, Okino L. Outcome study of bilateral lateral rectus recession for intermittent exotropia in children. Ophthalmic Surg Lasers. 1999; 30:110–117.15. Maruo T, Kubota N, Sakaue T, Usui C. Intermittent exotropia surgery in children: long term outcome regarding changes in binocular alignment. A study of 666 cases. Binocul Vis Strabismus Q. 2001; 16:265–270.16. Lee S, Lee YC. Relationship between motor alignment at postoperative day 1 and at year 1 after symmetric and asymmetric surgery in intermittent exotropia. Jpn J Ophthalmol. 2001; 45:167–171.17. Jeoung JW, Lee MJ, Hwang JM. Bilateral lateral rectus recession versus unilateral recess-resect procedure for exotropia with a dominant eye. Am J Ophthalmol. 2006; 141:683–688.18. Chia A, Seenyen L, Long QB. Surgical experiences with two-muscle surgery for the treatment of intermittent exotropia. J AAPOS. 2006; 10:206–211.19. Fiorelli VM, Goldchmit M, Uesugui CF, Souza-Dias C. Intermittent exotropia: comparative surgical results of lateral recti-recession and monocular recess-resect. Arq Bras Oftalmol. 2007; 70:429–432.20. Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. Postoperative outcomes in children with intermittent exotropia from a population-based cohort. J AAPOS. 2009; 13:4–7.21. Choi J, Chang JW, Kim SJ, Yu YS. The long-term survival analysis of bilateral lateral rectus recession versus unilateral recession-resection for intermittent exotropia. Am J Ophthalmol. 2012; 153:343–351.e1.22. Wang L, Wu Q, Kong X, Li Z. Comparison of bilateral lateral rectus recession and unilateral recession resection for basic type intermittent exotropia in children. Br J Ophthalmol. 2013; 97:870–873.23. Yang X, Man TT, Tian QX, et al. Long-term postoperative outcomes of bilateral lateral rectus recession vs unilateral recession-resection for intermittent exotropia. Int J Ophthalmol. 2014; 7:1043–1047.24. Saleem QA, Cheema AM, Tahir MA, et al. Outcome of unilateral lateral rectus recession and medial rectus resection in primary exotropia. BMC Res Notes. 2013; 6:257.25. Wright KW. Practical aspects of the adjustable suture technique for strabismus surgery. Int Ophthalmol Clin. 1989; 29:10–15.26. Burian HM, Spivey BE. The surgical management of exodeviations. Am J Ophthalmol. 1965; 59:603–620.27. Lim SH, Hong JS, Kim MM. Prognostic factors for recurrence with unilateral recess-resect procedure in patients with intermittent exotropia. Eye (Lond). 2011; 25:449–454.28. Lim SH, Hwang BS, Kim MM. Prognostic factors for recurrence after bilateral rectus recession procedure in patients with intermittent exotropia. Eye (Lond). 2012; 26:846–852.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Surgical Results between Bilateral and Unilateral Lateral Rectus Recession in 20~25 Prism Diopters Intermittent Exotropia
- Changes in Types of Recurrent Intermittent Exotropia after Surgical Correction of Basic Type Intermittent Exotropia
- How to Better Treat Patients with Intermittent Exotropia: A Review of Surgical Treatment of Intermittent Exotropia
- Comparison of Surgical Results between Bilateral Recession and Unilateral Recession-Resection in 25 PD Intermittent Exotropia
- The Effect of Unilateral Medial Rectus Muscle Resection in Patients with Recurrent Exotropia
