Clinical Features of Pregnancy-associated Retinal and Choroidal Diseases Causing Acute Visual Disturbance
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. sejoon1@snu.ac.kr
- 2Department of Ophthalmology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2385581
- DOI: http://doi.org/10.3341/kjo.2016.0080
Abstract
- PURPOSE
To report clinical features of patients with retinal and choroidal diseases presenting with acute visual disturbance during pregnancy.
METHODS
In this retrospective case series, patients who developed acute visual loss during pregnancy (including puerperium) and visited a tertiary hospital from July 2007 to June 2015, were recruited by searching electronic medical records. Patients were categorized according to the cause of visual loss. Clinical features and required diagnostic modalities were analyzed in the retinal and choroidal disease group.
RESULTS
Acute visual loss occurred in 147 patients; 49 (38.9%) were classified into the retinal and choroidal group. The diagnoses included central serous chorioretinopathy (22.4%), hypertensive retinopathy with or without pre-eclampsia (22.4%), retinal tear with or without retinal detachment (18.4%), diabetic retinopathy progression (10.2%), Vogt-Koyanagi-Harada disease (4.1%), retinal artery occlusion (4.1%), multiple evanescent white dot syndrome (4.1%), and others (14.3%). Visual symptoms first appeared at gestational age 25.9 ± 10.3 weeks. The initial best-corrected visual acuity (BCVA) was 0.27 ± 0.39 logarithm of the minimum angle of resolution (logMAR); the final BCVA after delivery improved to 0.13 ± 0.35 logMAR. Serious visual deterioration (BCVA worth than 20 / 200) developed in two patients. Differential diagnoses were established with characteristic fundus and spectral-domain optical coherence tomography findings in all cases.
CONCLUSIONS
In pregnant women with acute visual loss, retinal and choroidal diseases are common and could be vision threatening. Physicians should be aware of pregnancy-associated retinal and choroidal diseases and their clinical features. The differential diagnosis can be established with non-invasive techniques.
Keyword
MeSH Terms
-
Central Serous Chorioretinopathy
Choroid Diseases*
Choroid*
Diabetic Retinopathy
Diagnosis
Diagnosis, Differential
Electronic Health Records
Female
Gestational Age
Humans
Hypertensive Retinopathy
Pre-Eclampsia
Pregnancy
Pregnant Women
Retinal Artery Occlusion
Retinal Detachment
Retinal Diseases
Retinal Perforations
Retinaldehyde*
Retrospective Studies
Tertiary Care Centers
Tomography, Optical Coherence
Uveomeningoencephalitic Syndrome
Visual Acuity
Retinaldehyde
Figure
-

Fig. 1 Search process for the subject group. CNS = central nervous system.

Fig. 2 Optical coherence tomography images in enhanced depth image mode of a patient who was diagnosed with central serous chorioretinopathy at gestational age 25 weeks. (A) The image obtained at gestational age 25 weeks. The dilated large choroidal vessels (arrows), which are characteristic of central serous chorioretinopathy, are visible. (B) The image obtained at 2 weeks postpartum.

Fig. 3 Sequential images of a patient who was diagnosed with and underwent treatment for high-risk proliferative diabetic retinopathy during pregnancy (the sequential images were obtained at gestational age (GA) 22 weeks, GA 29 weeks, 5 weeks postpartum, and 10 weeks postpartum). This patient underwent panretinal photocoagulation at GA 22 weeks and received intravitreal injection of bevacizumab at GA 29 weeks. Wide-angle fundus photographs show rapid progression of tractional membrane and the development of preretinal hemorrhage, and the optical coherence tomography images show aggravation and relief of diabetic macular edema. The patient underwent pars plana vitrectomy for tractional retinal detachment 7 months after delivery.
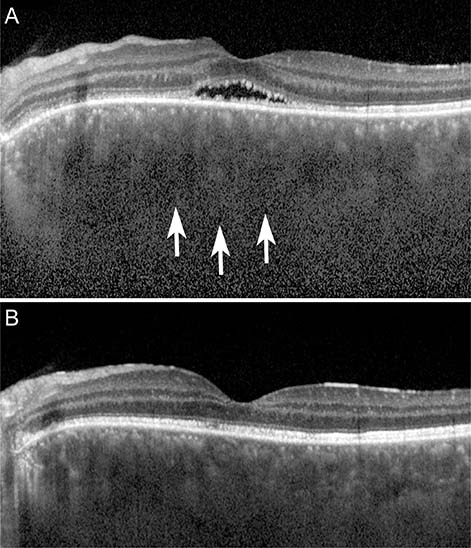
Fig. 4 Images of a patient diagnosed with incomplete Vogt-Koyanagi-Harada during pregnancy. (A) Enhanced depth image optical coherence tomography image of the left eye at gestational age 20 weeks revealing serous retinal detachment with subretinal exudation and choroidal thickening (arrows). (B) Enhanced depth image optical coherence tomography image at gestational age 22 weeks revealing that the subretinal fluid resolved after administration of systemic corticosteroid.

Fig. 5 Fundus photograph and optical coherence tomography image of patient 14, who was diagnosed with central retinal artery occlusion at gestational age 18 weeks. The images were obtained 1 week after the onset of the event, and the acute ischemic changes of the inner retina are apparent.
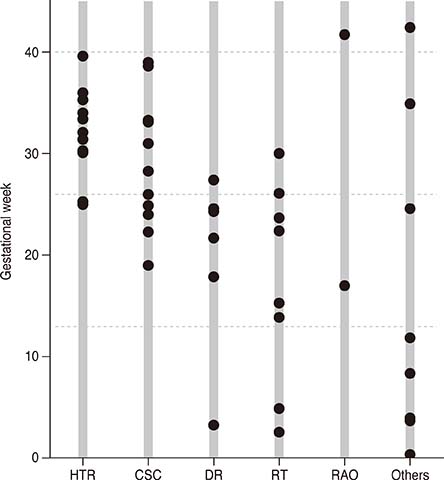
Fig. 6 Initial symptom onset in each disease category. HTR = hypertensive retinopathy; CSC = central serous chorioretinopathy; DR = diabetic retinopathy; RT = retinal tear with or without retinal detachment; RAO = retinal artery occlusion. Symptom onset was significantly different in the HTR group compared with that in the other disease groups (p = 0.002 by the Mann-Whitney U-test), but no differences were observed with the other groups.
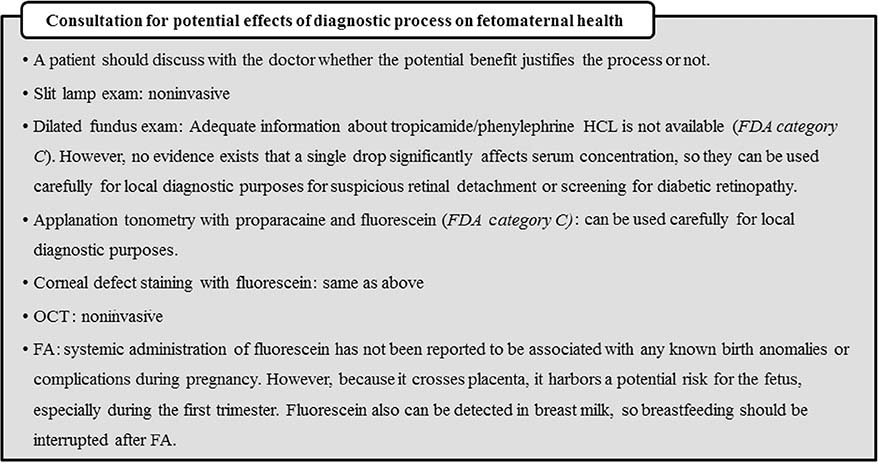
Fig. 7 Consultation for potential effects of diagnostic process on fetomaternal health [1112]. HCl = phenylephrine hydrochloride; FDA = Food and Drug Administration (United States); OCT = optical coherence tomography; FA = fluorescein angiography
Reference
-
1. Errera MH, Kohly RP, da Cruz L. Pregnancy-associated retinal diseases and their management. Surv Ophthalmol. 2013; 58:127–142.2. Thornburg KL, Jacobson SL, Giraud GD, Morton MJ. Hemodynamic changes in pregnancy. Semin Perinatol. 2000; 24:11–14.3. Schocket LS, Grunwald JE, Tsang AF, DuPont J. The effect of pregnancy on retinal hemodynamics in diabetic versus nondiabetic mothers. Am J Ophthalmol. 1999; 128:477–484.4. Saito Y, Tano Y. Retinal pigment epithelial lesions associated with choroidal ischemia in preeclampsia. Retina. 1998; 18:103–108.5. Doi M, Matsubara H, Uji Y. Vogt-Koyanagi-Harada syndrome in a pregnant patient treated with high-dose systemic corticosteroids. Acta Ophthalmol Scand. 2000; 78:93–96.6. Rabiah PK, Vitale AT. Noninfectious uveitis and pregnancy. Am J Ophthalmol. 2003; 136:91–98.7. Acheson JF, Gregson RM, Merry P, Schulenburg WE. Vaso-occlusive retinopathy in the primary anti-phospholipid antibody syndrome. Eye (Lond). 1991; 5(Pt 1):48–55.8. Greven CM, Weaver RG, Owen J, Slusher MM. Protein S deficiency and bilateral branch retinal artery occlusion. Ophthalmology. 1991; 98:33–34.9. Sim DA, Sheth HG, Kaines A, Tufail A. Punctate inner choroidopathy-associated choroidal neovascular membranes during pregnancy. Eye (Lond). 2008; 22:725–727.10. Grant AD, Chung SM. The eye in pregnancy: ophthalmologic and neuro-ophthalmologic changes. Clin Obstet Gynecol. 2013; 56:397–412.11. Mackensen F, Paulus WE, Max R, Ness T. Ocular changes during pregnancy. Dtsch Arztebl Int. 2014; 111:567–575.12. American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 2001; 108:776–789.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Visual Improvement following Acute Obstruction of the Retinal and Choroidal Blood Flows
- Spontaneous resolution of serous retinal detachment caused by choroidal mass after a first trimester abortion
- Clinical Evaluation of Choroidal Detachment Associated with Rhegmatogenous Retinal Detachment
- A Case of Retinal Contusion Combined Exudative Retinal Detachment Causing Delayed Visual Disturbance
- Laser Photocoaculation Treatment in a Case of Circumscribged Choroidal hmangioma Associated with Serous Retinal Detachment
