Trend of CD4+ Cell Counts at Diagnosis and Initiation of Highly Active Antiretroviral Therapy (HAART): Korea HIV/AIDS Cohort Study, 1992-2015
- Kim MJ

- Chang HH
- Kim SI
- Kim YJ
- Park DW
- Kang C
- Kee MK
- Choi JY
- Kim SM
- Choi BY
- Kim WJ
- Kim JM
- Choi JY
- Choi YH
- Lee JS
- Kim SW
- Korea HIV/AIDS Cohort Study
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University, Daegu, Korea. ksw2kms@knu.ac.kr
- 2Division of Infectious Diseases, Department of Internal Medicine, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 3Division of Infectious Diseases, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- 4Division of AIDS, Korea Centers for Disease Control and Prevention, Cheongju, Korea.
- 5Institute for Health and Society, Hanyang University, Seoul, Korea.
- 6Department of Preventive Medicine, Hanyang University College of Medicine, Seoul, Korea.
- 7Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- 8Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 9AIDS Research Institute, Yonsei University College of Medicine, Seoul, Korea.
- 10Department of Infectious Diseases, Ajou University School of Medicine, Suwon, Korea.
- 11Department of Internal Medicine, Inha University School of Medicine, Incheon, Korea.
- KMID: 2383930
- DOI: http://doi.org/10.3947/ic.2017.49.2.101
Abstract
- BACKGROUND
CD4+ cell counts reflect immunologic status of human immunodeficiency virus (HIV) patients. Recommended CD4+ cell counts for the initiation of highly active antiretroviral therapy (HAART) has increased over the past several years in various HIV treatment guidelines. We investigated the trend of CD4+ cell counts at diagnosis and treatment start using data from the Korea HIV/acquired immune deficiency syndrome (AIDS) Cohort Study.
MATERIALS AND METHODS
The Korea HIV/AIDS Cohort Study started in 2006 and enrolled HIV patients from 21 tertiary and secondary hospitals in South Korea. The data for CD4+ cell counts at diagnosis and HAART initiation from these HIV patients were analyzed by three-year time intervals and presented by number of CD4+ cells (≤100, 101-200, 201-350, 351-500 and >500 cells/mm³). The HIV-RNA titer at diagnosis and HAART initiation were presented by 3-year intervals by groups ≤50,000, 50,001-100,000, 100,001-200,000, 200,001-1,000,000, and >1,000,000 copies/mL.
RESULTS
Median values of CD4+ cell count and HIV-RNA titer at initial HIV diagnosis were 247 cells/mm³ and 394,955 copies/mL, respectively. At time of initiating HAART, median values of CD4+ cell count and HIV-RNA were 181 cells/mm³ and 83,500 copies/mL, respectively. Patients with low CD4+ cell count (CD4+ cell count ≤200 cells/mm³) at diagnosis (31-51%) and initiation of HAART accounted for the largest proportion (30-65%) over the three-year time intervals. This proportion increased until 2010-2012.
CONCLUSION
CD4+ cell count at initiation of HAART was found to be very low, and the increase in late initiation of HAART in recent years is of concern. We think that this increase is primarily due to an increasing proportion of late presenters. We recommend early detection of HIV patients and earlier start of HAART in order to treat and prevent spread of HIV infection.
MeSH Terms
Figure
-

Figure 1 The trend of CD4+ cell count at the time of diagnosis by 3-year intervals. As of 2015, a total of 1,124 HIV-infected patients were included. Each period was stratified by grade of CD4+ cell count: ≤100, 101-200, 201-350, 351-500, and >500 cells/mm3. Values are presented as number (percentage).
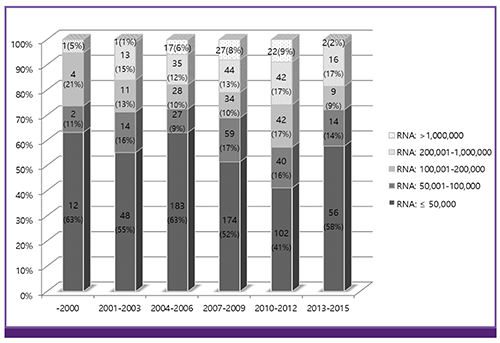
Figure 2 The trend of HIV-RNA titer at the time of diagnosis by 3-year intervals. As of 2015, a total of 1,079 HIV-infected patients were included. Each period was stratified by the level of HIV-RNA titer: ≤50,000, 500,001-100,000, 100,001-200,000, 200,001-1,000,000, and >1,000,000 copies/mL. Values are presented as number (percentage).

Figure 3 The trend of CD4+ cell count at the time of initiating highly active antiretroviral therapy by 3-year intervals. As of 2015, 376 HIV patients were included. CD4+ cell count, ≤100, 101-200, 201-350, 351-500, and >500 cells/mm3, is stratified for each time interval. Values are presented as number (percentage).
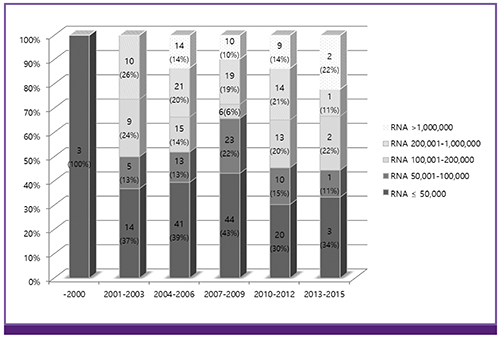
Figure 4 The trend of HIV-RNA titer at the time of initiating highly active antiretroviral therapy by three-year intervals. As of 2015, 322 HIV patients were included. Level of HIV-RNA: ≤50,000; 50,001-100,000; 100,001-200,000; 200,001-1,000,000; and >1,000,000 copies/mL is stratified for each time interval. Values are presented as number (percentage).
Cited by 3 articles
-
Significance of Increased Rapid Treatment from HIV Diagnosis to the First Antiretroviral Therapy in the Recent 20 Years and Its Implications: the Korea HIV/AIDS Cohort Study
Yoon-Jung Kim, Shin-Woo Kim, Ki Tae Kwon, Hyun-Ha Chang, Sang Il Kim, Youn Jeong Kim, Min Ja Kim, Jun Yong Choi, Hyo Youl Kim, June Myung Kim, Bo Youl Choi, Bo Young Park, Yun Su Choi, Mee-Kyung Kee, Myeong Su Yoo, Jung Gyu Lee
J Korean Med Sci. 2019;34(38):. doi: 10.3346/jkms.2019.34.e239.Trend in CD4+ Cell Counts at Diagnosis in Human Immunodeficiency Virus-Infected Persons in Korea
Nam Joong Kim
Infect Chemother. 2017;49(2):155-157. doi: 10.3947/ic.2017.49.2.155.Human Immunodeficiency Virus (HIV) and Hepatitis Virus Coinfection among HIV-Infected Korean Patients: The Korea HIV/AIDS Cohort Study
Yong Chan Kim, Jin Young Ahn, June Myung Kim, Youn Jeong Kim, Dae Won Park, Young Kyung Yoon, Joon Young Song, Shin Woo Kim, Jin Soo Lee, Bo Youl Choi, Yun Su Choi, Ju-yeon Choi, Myung Guk Han, Chun Kang, Jun Yong Choi
Infect Chemother. 2017;49(4):268-274. doi: 10.3947/ic.2017.49.4.268.
Reference
-
1. Hermans SM, van Leth F, Manabe YC, Hoepelman AI, Lange JM, Kambugu A. Earlier initiation of antiretroviral therapy, increased tuberculosis case finding and reduced mortality in a setting of improved HIV care: a retrospective cohort study. HIV Med. 2012; 13:337–344.
Article2. Kiertiburanakul S, Boettiger D, Lee MP, Omar SF, Tanuma J, Ng OT, Durier N, Phanuphak P, Ditangco R, Chaiwarith R, Kantipong P, Lee CK, Mustafa M, Saphonn V, Ratanasuwan W, Merati TP, Kumarasamy N, Wong WW, Zhang F, Pham TT, Pujari S, Choi JY, Yunihastuti E, Sungkanuparph S. TREAT Asia HIV Observational Databases (TAHOD). TREAT Asia Studies to Evaluate Resistance (TASER). Trends of CD4 cell count levels at the initiation of antiretroviral therapy over time and factors associated with late initiation of antiretroviral therapy among Asian HIV-positive patients. J Int AIDS Soc. 2014; 17:18804.
Article3. World Health Organization (WHO). Fact sheet: 2014 statistics. Accessed 24 August 2015. Available at: http://www.unaids.org/en/resources/documents/2015/20150714_factsheet.4. Asfaw A, Ali D, Eticha T, Alemayehu A, Alemayehu M, Kindeya F. CD4 cell count trends after commencement of antiretroviral therapy among HIV-infected patients in Tigray, Northern Ethiopia: a retrospective cross-sectional study. PLoS One. 2015; 10:e0122583.
Article5. Yamashita TE, Phair JP, Muñoz A, Margolick JB, Detels R, O’Brien SJ, Mellors JW, Wolinsky SM, Jacobson LP. Immunologic and virologic response to highly active antiretroviral therapy in the Multicenter AIDS Cohort Study. AIDS. 2001; 15:735–746.
Article6. Kelley CF, Kitchen CM, Hunt PW, Rodriguez B, Hecht FM, Kitahata M, Crane HM, Willig J, Mugavero M, Saag M, Martin JN, Deeks SG. Incomplete peripheral CD4+ cell count restoration in HIV-infected patients receiving long-term antiretroviral treatment. Clin Infect Dis. 2009; 48:787–794.
Article7. Baker JV, Peng G, Rapkin J, Abrams DI, Silverberg MJ, MacArthur RD, Cavert WP, Henry WK, Neaton JD. Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA). CD4+ count and risk of non-AIDS diseases following initial treatment for HIV infection. AIDS. 2008; 22:841–848.
Article8. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG, Kumwenda J, Grinsztejn B, Pilotto JH, Godbole SV, Mehendale S, Chariyalertsak S, Santos BR, Mayer KH, Hoffman IF, Eshleman SH, Piwowar-Manning E, Wang L, Makhema J, Mills LA, de Bruyn G, Sanne I, Eron J, Gallant J, Havlir D, Swindells S, Ribaudo H, Elharrar V, Burns D, Taha TE, Nielsen-Saines K, Celentano D, Essex M, Fleming TR; HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011; 365:493–505.
Article9. European AIDS Clinical Society (EACS). The European Guidelines for treatment of HIV infected adults in Europe. Accessed 4 November 2015. Available at: http://www.eacsociety.org/files/2015_eacsguidelines_8.0-english_revised-20151104.pdf.10. Department of Health and Human Services (HHS). Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Accessed 8 April 2015. Available at: https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf.11. World Health Organization (WHO). Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Accessed 30 September 2015. Available at: http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf.12. The Korean Society for AIDS. The 2013 clinical guidelines for the diagnosis and treatment of HIV/AIDS in HIV-infected Koreans. Infect Chemother. 2013; 45:455–461.13. Kiertiburanakul S, Boonyarattaphun K, Atamasirikul K, Sungkanuparph S. Clinical presentations of newly diagnosed HIV-infected patients at a university hospital in Bangkok, Thailand. J Int Assoc Physicians AIDS Care (Chic). 2008; 7:82–87.
Article14. Korean Society for AIDS. The 2015 clinical guidelines for the treatment and prevention of opportunistic infections in HIV-infected Koreans: guidelines for opportunistic infections. Infect Chemother. 2016; 48:54–60.15. Kee MK, Lee JH, Kim GJ, Choi BS, Hong KJ, Lee JS, Kim SS. Decrease of initial CD4+ T-cell counts at the time of diagnosis of HIV infection in Korea; 1988-2006. Int J STD AIDS. 2010; 21:120–125.
Article16. Pernas B, Mena A, Cañizares A, Grandal M, Castro-Iglesias A, Pértega S, Pedreira JD, Poveda E. Trends on epidemiological, virological, and clinical features among newly diagnosed HIV-1 persons in Northwest Spain over the last 10 years. J Med Virol. 2015; 87:1319–1326.
Article17. Delpech V, Brown AE, Croxford S, Chau C, Polavarapu V, Cooper N, Rooney G, Yin Z. Quality of HIV care in the United Kingdom: key indicators for the first 12 months from HIV diagnosis. HIV Med. 2013; 14:Suppl 3. 19–24.
Article18. Shen Y, Lu H, Wang Z, Qi T, Wang J. Analysis of the immunologic status of a newly diagnosed HIV positive population in China. BMC Infect Dis. 2013; 13:429.
Article19. Shen Y, Wang J, Qi T, Wang Z, Lu H. Trends in clinical characteristics of HIV-infected patients initiating antiretroviral therapy in Shanghai from 2006 to 2011. Int J STD AIDS. 2013; 25:504–510.
Article20. Mutimura E, Addison D, Anastos K, Hoover D, Dusingize JC, Karenzie B, Izimukwiye I, Mutesa L, Nsanzimana S, Nash D. IeDEA Central Africa Collaboration. Trends in and correlates of CD4+ cell count at antiretroviral therapy initiation after changes in national ART guidelines in Rwanda. AIDS. 2015; 29:67–76.
Article21. Miranda AC, Moneti V, Brogueira P, Peres S, Baptista T, Aldir I, Ventura F, Borges F, Mansinho K. Evolution trends over three decades of HIV infection late diagnosis: the experience of a Portuguese cohort of 705 HIV-infected patients. J Int AIDS Soc. 2014; 17:Suppl 3. 19688.
Article22. Lesko CR, Cole SR, Zinski A, Poole C, Mugavero MJ. A systematic review and meta-regression of temporal trends in adult CD4(+) cell count at presentation to HIV care, 1992-2011. Clin Infect Dis. 2013; 57:1027–1037.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of systemic inflammatory reactions after highly active antiretroviral therapy in HIV infected patients with tuberculosis
- Therapeutic Response of HAART and Analysis of Related Factors in Korean HIV-infected Persons
- The CD4 slope can be a predictor of immunologic recovery in advanced HIV patients: a case-control study
- Frequency of Skin Disorders in HIV-infected Patients and Their Relationship to CD4+ T Lymphocyte Counts
- Factors Associated with HIV-1 Proviral DNA Loads in Patients with Undetectable Plasma RNA Load
