Clin Endosc.
2017 Mar;50(2):191-196. 10.5946/ce.2016.093.
Persistent Nonbilious Vomiting in a Child: Possible Duodenal Webbing
- Affiliations
-
- 1Division of Pediatric Surgery, Department of Medical, Surgical and Neurological Sciences, University of Siena, Siena, Italy. rossellaangotti@me.com
- 2Pediatric Surgery Unit, Academic Salesi Children Hospital, Marche Polytechnic University, Ancona, Italy.
- 3Section of Obstetrics and Gynecology, Department of Molecular and Developmental Medicine, University of Siena, Siena, Italy.
- KMID: 2383537
- DOI: http://doi.org/10.5946/ce.2016.093
Abstract
- An association between malrotation and congenital duodenal webbing is rare. We present our experience with four patients at two centers, and a review of published reports. There are currently 94 reported cases of duodenal pathology associated with malrotation. However, only 15 of the 94 cases (15.9%) include patients with malrotation and a duodenal web. We suggest that nonbilious vomiting in a child must prompt the surgeon to consider duodenal pathology even in the presence of malrotation.
Figure
-
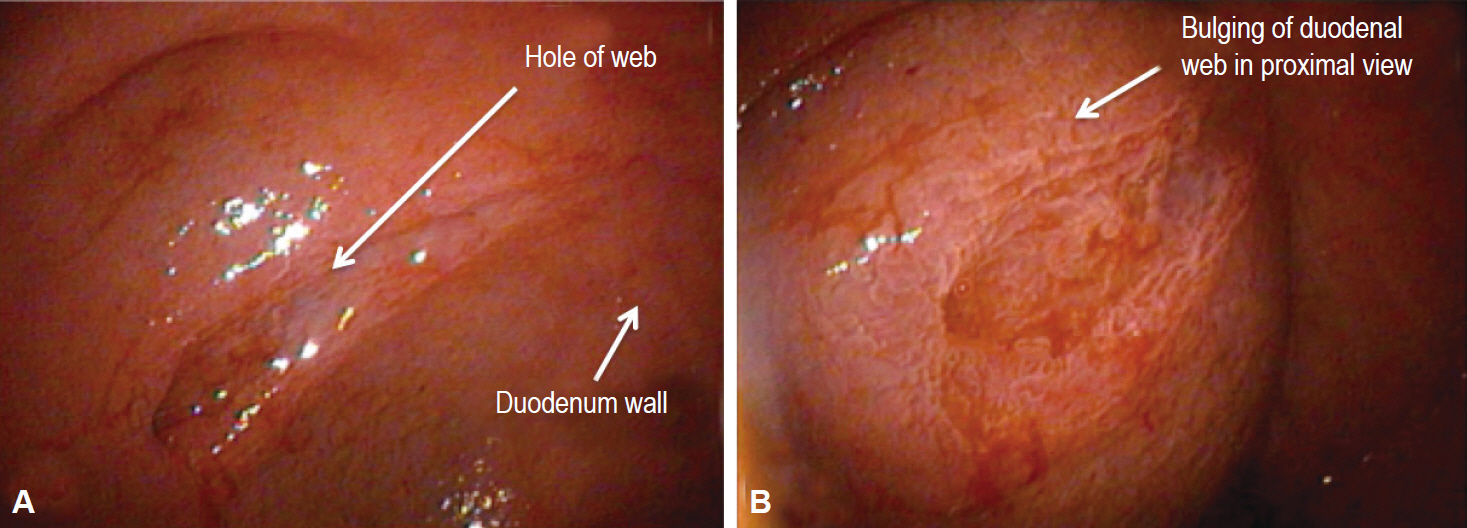
Fig. 1. Case 1: 2-year-old girl. (A, B) An endoscopic picture of her congenital duodenal web. This is a view during an endoscopic procedure. (B) The tag shows the bulging of the duodenal web.

Fig. 2. Case 3: 10-year-old girl. (A, B) An upper gastrointestinal contrast study shows a duodenal stenosis with delayed emptying of the 2nd duodenal portion (red arrow) and all of the small bowel in the right quadrant and the colon in the left quadrant because of a previous Valdoni’s procedure.
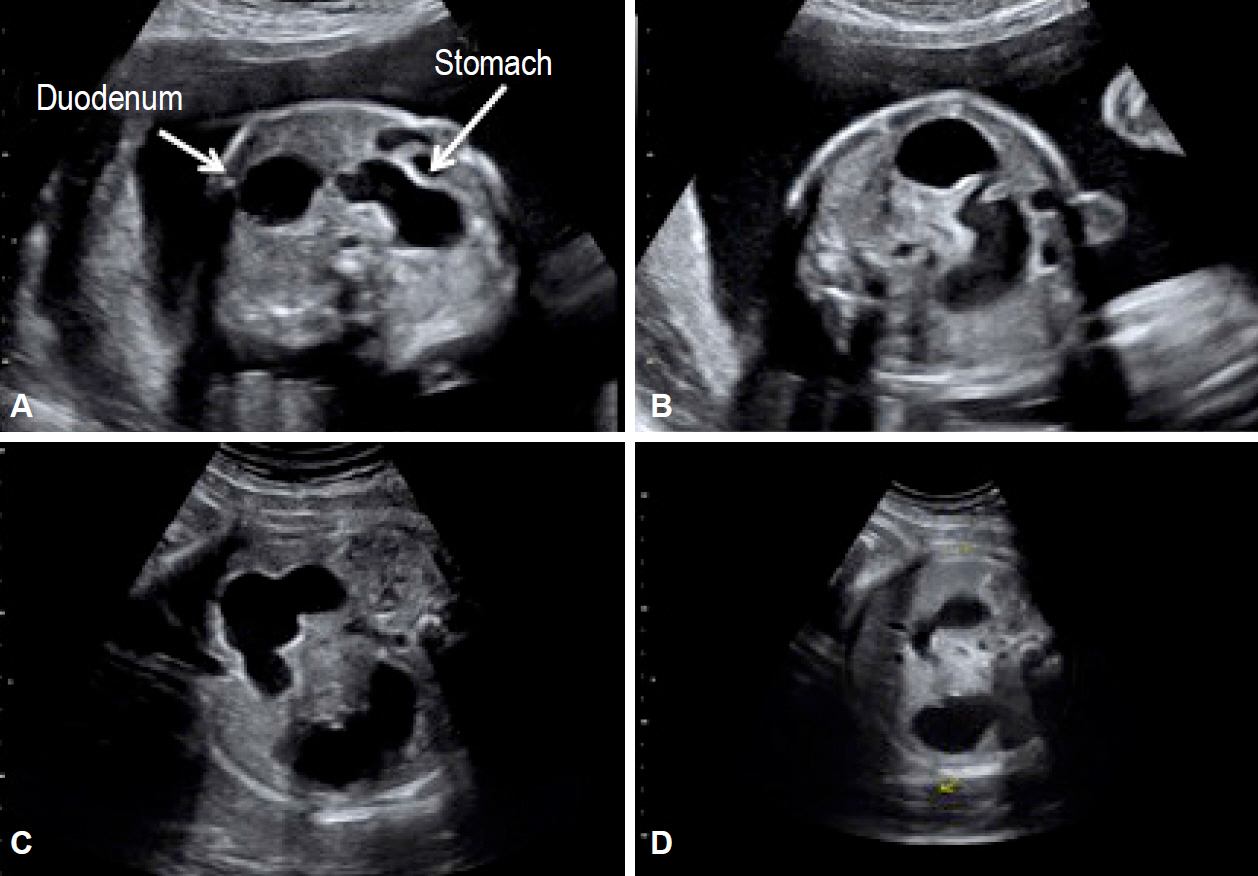
Fig. 3. Case 4. (A-D) Prenatal ultrasound shows the presence of a double bubble that was suspected to be a duodenal pathology.
Reference
-
1. Ingoe R, Lange P. The Ladd’s procedure for correction of intestinal malrotation with volvulus in children. AORN J. 2007; 85:300–308.2. Angotti R, Bulotta AL, Ferrara F, et al. Uncommon surgical emergencies in neonatology. Pediatr Med Chir. 2014; 36:99.
Article3. Beeks A, Gosche J, Giles H, Nowicki M. Endoscopic dilation and partial resection of a duodenal web in an infant. J Pediatr Gastroenterol Nutr. 2009; 48:378–381.
Article4. Sweed Y. Duodenal obstruction. In : Puri P, Höllwarth ME, editors. Pediatric Surgery: Diagnosis and Management. London: Springer;2009. p. 383–392.5. Lampl B, Levin TL, Berdon WE, Cowles RA. Malrotation and midgut volvulus: a historical review and current controversies in diagnosis and management. Pediatr Radiol. 2009; 39:359–366.
Article6. Penco JM, Murillo JC, Hernández A, De La Calle Pato U, Masjoan DF, Aceituno FR. Anomalies of intestinal rotation and fixation: consequences of late diagnosis beyond two years of age. Pediatr Surg Int. 2007; 23:723–730.
Article7. Yoon CH, Goo HW, Kim EA, Kim KS, Pi SY. Sonographic windsock sign of a duodenal web. Pediatr Radiol. 2001; 31:856–857.
Article8. Madding GF, Everhart MW, Heath J. Congenital duodenal atresia with malrotation of the intestine; a case successfully treated by duodeno-jejunostomy. Ann Surg. 1950; 131:433–436.9. Baumgartner F, Moore TC. Atretic, obstructive proximal duodenal mass associated with annular pancreas and malrotation in a newborn male. Eur J Pediatr Surg. 1992; 2:42–44.
Article10. Barrack SM, Kyambi JM, Ndungu J, Wachira N, Anangwe G, Safwat S. Intestinal atresia and stenosis as seen and treated at Kenyatta National Hospital, Nairobi. East Afr Med J. 1993; 70:558–564.11. Zerin JM, Polley TZ Jr. Malrotation in patients with duodenal atresia: a true association or an expected finding on postoperative upper gastrointestinal barium study? Pediatr Radiol. 1994; 24:170–172.
Article12. Samuel M, Wheeler RA, Mami AG. Does duodenal atresia and stenosis prevent midgut volvulus in malrotation? Eur J Pediatr Surg. 1997; 7:11–12.
Article13. Dalla Vecchia LK, Grosfeld JL, West KW, Rescorla FJ, Scherer LR, Engum SA. Intestinal atresia and stenosis: a 25-year experience with 277 cases. Arch Surg. 1998; 133:490–496.14. Chandran H, Upadhyay V, Pease PW. Multiple organ malrotation syndrome with duodenal atresia: a case report. Pediatr Surg Int. 1999; 15:61–62.
Article15. Pumberger W, Birnbacher R, Pomberger G, Deutinger J. Duodeno-jejunal atresia with volvulus, absent dorsal mesentery, and absent superior mesenteric artery: a hereditary compound structure in duodenal atresia? Am J Med Genet. 2002; 109:52–55.
Article16. Glüer S, Petersen C, Ure BM. Simultaneous correction of duodenal atresia due to annular pancreas and malrotation by laparoscopy. Eur J Pediatr Surg. 2002; 12:423–425.
Article17. Aslanabadi S, Ghalehgolab-Behbahan A, Jamshidi M, Veisi P, Zarrintan S. Intestinal malrotations: a review and report of thirty cases. Folia Morphol (Warsz). 2007; 66:277–282.18. Morikawa N, Kuroda T, Honna T, et al. A novel association of duodenal atresia, malrotation, segmental dilatation of the colon, and anorectal malformation. Pediatr Surg Int. 2009; 25:1003–1005.
Article19. Patil RT, Gupta R, Parelkar SV, et al. A rare case of duodenal atresia with apple-peel configuration of the small intestine and malrotation. Eur J Pediatr Surg. 2011; 21:340–342.
Article20. Eksarko P, Nazir S, Kessler E, et al. Duodenal web associated with malrotation and review of literature. J Surg Case Rep. 2013; 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Diagnosis of Duodenal Stenosis in a 5-Month-Old Male Infant
- A Case of Duodenal Web Associated with Intestinal Malrotation
- Duodenal Obstruction due to Duodenal Web in Three-year-old Girl: A Case Report
- Heterotopic Pancreas Presented as Duodenal Tumor with Obstruction
- Congenital Duodenal Web Associated with a Foreign Body (Go Stone) in a 10-Year-Old Girl
