Multidrug-Resistant Tuberculous Mediastinal Lymphadenitis, with an Esophagomediastinal Fistula, Mimicking an Esophageal Submucosal Tumor
- Affiliations
-
- 1Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. stomachlee@gmail.com
- KMID: 2383454
- DOI: http://doi.org/10.5946/ce.2016.020
Abstract
- Mediastinal tuberculous lymphadenitis rarely mimics esophageal submucosal tumor, particularly in the case of multidrug-resistant tuberculosis (MDR-TB). Herein, we report the case of a 61-year-old woman who visited a local hospital complaining of odynophagia. An initial esophagogastroduodenoscopy revealed an esophageal submucosal tumor, and subsequent chest computed tomography showed subcarinal lymphadenopathy with an esophagomediastinal fistula. The patient was then referred to Samsung Medical Center, and a second esophagogastroduodenoscopy showed deep central ulceration, as well as a suspicious fistula in the esophageal submucosal tumor-like lesion. A biopsy examination of the ulcerative lesion confirmed focal inflammation only. Next, an endobronchial, ultrasound-guided lymph node biopsy was performed, and TB was confirmed. The patient initially began a course of isoniazid, rifampicin, ethambutol, and pyrazinamide. However, after a drug sensitivity test, she was diagnosed with MDR-TB, and second-line anti-TB medications were prescribed. She recovered well subsequently.
Keyword
MeSH Terms
Figure
-

Fig. 1. (A, B) Initial esophagogastroduodenoscopic view of the esophageal submucosal tumor-like lesion (arrow) 27 cm from the upper incisor.
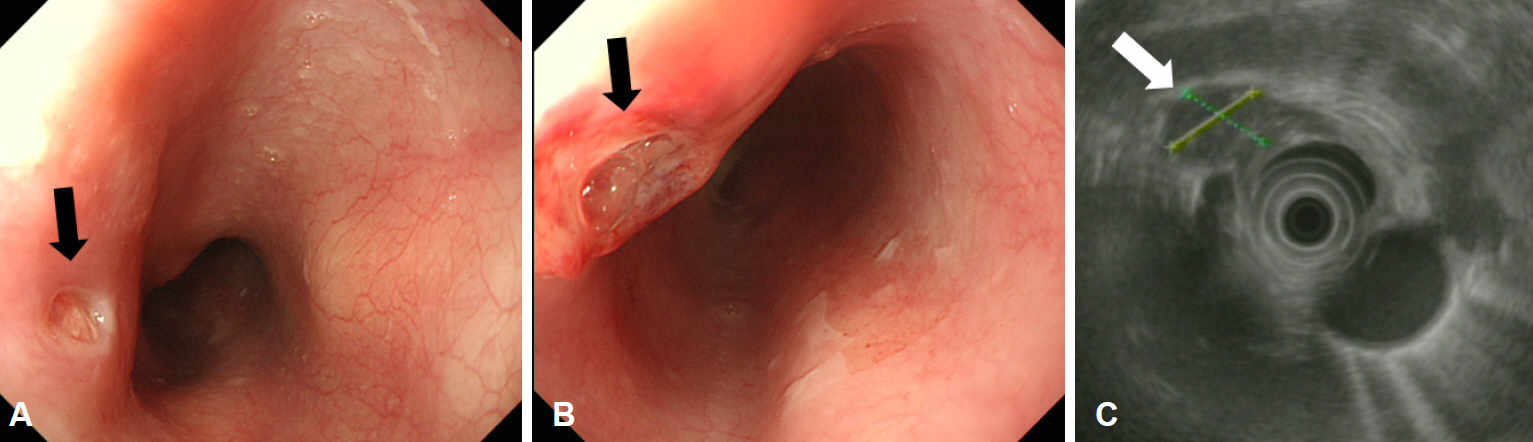
Fig. 2. Endoscopic ultrasonographic findings 4 weeks after the initial presentation. (A, B) A submucosal tumor-like lesion with ulceration (arrows) can be seen 27 cm from the upper incisors. (C) It shows mixed echogenicity and an irregular margin, and the esophageal wall layer cannot be distinguished on endoscopic ultrasonography.

Fig. 3. (A, B) Chest contrast computed tomographic scan showing subcarinal lymphadenopathy with a probable fistulous connection to the esophageal lumen (arrows), (C) as well as paratracheal lymphadenopathy (arrow).
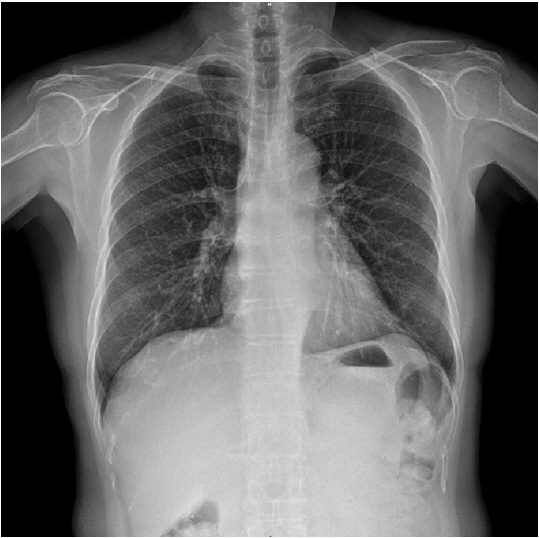
Fig. 4. An initial chest radiograph acquired at our hospital, showing normal chest findings.

Fig. 5. Chest computed tomography scan 3 months after initial presentation. The extent of mediastinal lymphadenopathy is increased along the (A) subcarinal (arrow), (B) para-aortic (arrow), and (C) paratracheal lymph nodes (arrow), and (D) a new branching nodular lesion can be seen in the left upper lobe of the lung (arrow), which suggests pulmonary tuberculosis.
Reference
-
1. Amorosa JK, Smith PR, Cohen JR, Ramsey C, Lyons HA. Tuberculous mediastinal lymphadenitis in the adult. Radiology. 1978; 126:365–368.
Article2. Ayed AK, Behbehani NA. Diagnosis and treatment of isolated tuberculous mediastinal lymphadenopathy in adults. Eur J Surg. 2001; 167:334–338.3. Shiota Y, Kitade M, Ueda N, Furuya K. Tuberculous mediastinal lymphadenitis in an adult patient. Jpn J Med. 1989; 28:382–384.
Article4. Ohtake M, Saito H, Okuno M, Yamamoto S, Ohgimi T. Esophagomediastinal fistula as a complication of tuberculous mediastinal lymphadenitis. Intern Med. 1996; 35:984–986.
Article5. Lin JN, Lai CH, Chen YH, et al. Risk factors for extra-pulmonary tuberculosis compared to pulmonary tuberculosis. Int J Tuberc Lung Dis. 2009; 13:620–625.6. Kim JH, Yim JJ. Achievements in and challenges of tuberculosis control in South Korea. Emerg Infect Dis. 2015; 21:1913–1920.
Article7. Adada H, Valley MA, Nour SA, et al. Epidemiology of extra-pulmonary tuberculosis in the United States: high rates persist in the post-HIV era. Int J Tuberc Lung Dis. 2014; 18:1516–1521.
Article8. Mou Y, Zeng H, Wang QM, et al. Esophageal tuberculosis initially misdiagnosed by endoscopy as a submucosal tumor. Endoscopy. 2015; 47 Suppl 1 UCTN:E30–E31.
Article9. Kang MJ, Yi SY. Esophageal tuberculosis presenting as a submucosal tumor. Clin Gastroenterol Hepatol. 2008; 6:A26.
Article10. Huang YK, Wu YC, Liu YH, Liu HP. Esophageal tuberculosis mimicking submucosal tumor. Interact Cardiovasc Thorac Surg. 2004; 3:274–276.
Article11. World Health Organization. Global tuberculosis report 2015 [Internet]. Geneva: World Health Organization;c2016. [cited 2016 Apr 5]. Available from: http://www.who.int/tb/publications/global_report/en/.12. Bai GH, Park YK, Choi YW, et al. Trend of anti-tuberculosis drug resistance in Korea, 1994-2004. Int J Tuberc Lung Dis. 2007; 11:571–576.13. Choi JC, Lim SY, Suh GY, et al. Drug resistance rates of Mycobacterium tuberculosis at a private referral center in Korea. J Korean Med Sci. 2007; 22:677–681.
Article14. Park HJ, Ryoo HM, Shin KC, et al. A clinical study of tuberculous lymphadenitis. Tuberc Respir Dis. 2000; 48:730–739.
Article15. Ko Y, Lee HY, Lee YS, et al. Esophagomediastinal fistula secondary to multidrug-resistant tuberculous mediastinal lymphadenitis. Intern Med. 2014; 53:1819–1824.
Article16. Geake J, Hammerschlag G, Nguyen P, et al. Utility of EBUS-TBNA for diagnosis of mediastinal tuberculous lymphadenitis: a multicentre Australian experience. J Thorac Dis. 2015; 7:439–448.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophago-Mediastinal Fistula Due to Tuberculous Mediastinal Lymphadenitis
- Dysphagia due to mediastinal tuberculous lymphadenitis presenting as an esophageal submucosal tumor: a case report
- A Case of Mediastinal Tuberculous Lymphadenitis Mimicking a Submucosal Tumor of the Esophagus
- A Case of Nontuberculous Mycobacterium Infection Complicated by an Esophagomediastinal Fistula in a Human Immunodeficiency Virus Patient
- Multidrug-resistant Tuberculosis Spondylitis: A Case Report
