Hepatobronchial Fistula and Lung Abscess after Transarterial Chemoembolization
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. dyk1025@yuhs.ac
- 2Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2383391
- DOI: http://doi.org/10.4166/kjg.2017.69.5.316
Abstract
- Transarterial chemoembolization (TACE) is a common treatment modality to locally manage hepatocellular carcinoma. Liver abscess and bile duct injury are common complications of TACE. However, hepatobronchial fistula is a rare complication. Herein, we report a case of lung abscess due to hepatobronchial fistula after TACE. A 67-year-old man, who had underwent TACE 6 months ago, presented cough and bile-colored sputum. He was diagnosed with lung abscess and hepatobronchial fistula. We performed endoscopic retrograde cholangiopancreatography; however, there was no improvement in his symptoms. Thereafter, partial hepatectomy and repair of fistula were successively conducted.
MeSH Terms
Figure
-

Fig. 1 Contrast-enhanced chest computed tomography at admission day. Hepatic abscess and lung abscess are shown in this image. The arrow indicates fistula between lung abscess and liver abscess.

Fig. 2 Cholangiography via hepatic abscess drainage catheter. The arrow indicates contrast dye leakage from hepatic abscess to bronchus.
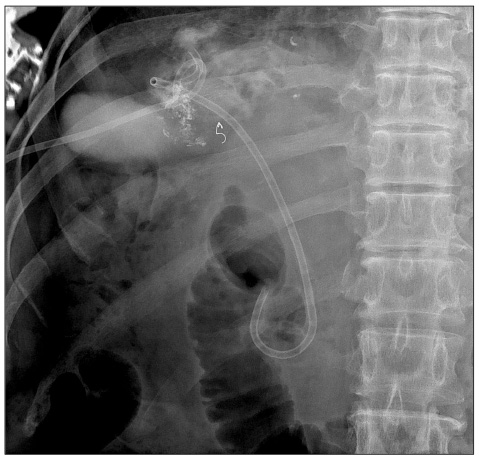
Fig. 3 Endoscopic retrograde cholangiopancreatography (ERCP) image. Endoscopic retrograde bile drainage was inserted via ERCP to treat hepatobronchial fistula by decompressing biliary pressure.

Fig. 4 Microscopic findings of the resected specimen (H&E, ×200). Postoperative pathology shows acute inflammation (neutrophil dominant) and necrosis.
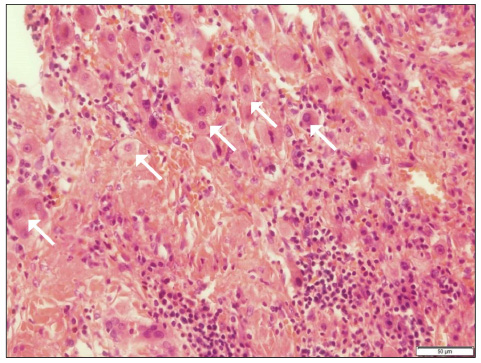
Fig. 5 Microscopic findings of the resected specimen (H&E, ×200). Postoperative pathology shows acute inflammation (neutrophil dominant) and some viable cancer cells (arrows).

Fig. 6 Liver-pelvic contrast dynamic computed tomography after repair operation. The arrow indicates repaired fistula at the diaphragm.
Reference
-
1. The Korean liver cancer study group, National cancer center. 2014 KLCSG-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Seoul (KR): 2014. 06. 14. updated 2014 Jun 14. cited Year 2015 Nov 24. Available from: http://www.klcsg.or.kr/html/sub03_02.asp.2. Paye F, Farges O, Dahmane M, Vilgrain V, Flejou JF, Belghiti J. Cytolysis following chemoembolization for hepatocellular carcinoma. Br J Surg. 1999; 86:176–180.3. Chung JW, Park JH, Han JK, et al. Hepatic tumors: predisposing factors for complications of transcatheter oily chemoembolization. Radiology. 1996; 198:33–40.4. Kim HK, Chung YH, Song BC, et al. Ischemic bile duct injury as a serious complication after transarterial chemoembolization in patients with hepatocellular carcinoma. J Clin Gastroenterol. 2001; 32:423–427.5. Marelli L, Stigliano R, Triantos C, et al. Transarterial therapy for hepatocellular carcinoma: which technique is more effective? A systematic review of cohort and randomized studies. Cardiovasc Intervent Radiol. 2007; 30:6–25.6. Song SY, Chung JW, Han JK, et al. Liver abscess after transcatheter oily chemoembolization for hepatic tumors: incidence, predisposing factors, and clinical outcome. J Vasc Interv Radiol. 2001; 12:313–320.7. Zhao H, Wang HQ, Fan QQ, Chen XX, Lou JY. Rare pulmonary and cerebral complications after transarterial chemoembolisation for hepatocellular carcinoma: a case report. World J Gastroenterol. 2008; 14:6425–6427.8. Kontoravdis N, Panagiotopoulos N, Lawrence D. The challenging management of hepatopulmonary fistulas. J Thorac Dis. 2014; 6:1336–1339.9. Liao GQ, Wang H, Zhu GY, Zhu KB, Lv FX, Tai S. Management of acquired bronchobiliary fistula: a systematic literature review of 68 cases published in 30 years. World J Gastroenterol. 2011; 17:3842–3849.10. Gulamhussein MA, Patrini D, Pararajasingham J, et al. Hepatopulmonary fistula: a life threatening complication of hydatid disease. J Cardiothorac Surg. 2015; 10:103.11. Korkmaz M, Bozkaya H, Çınar C, et al. Liver abscess following radioembolization with yttrium-90 microspheres. Wien Klin Wochenschr. 2014; 126:785–788.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of hepatobronchial fistula in liver abscess
- A Case of Transcatheter Arterial Embolization-nduced Hepatobronchial Fistula in a Patient with Hepatocellular Carcinoma
- A Case of Hepaticoduodenal Fistula Development after Transarterial Chemoembolization in Patient with Hepatocellular Carcinoma
- A Case of Pyogenic Liver Abscess Complicated by Hepatobronchial Fistula
- Rare Case of Pyogenic Brain Abscess after Transarterial Chemoembolization in a Patient with Hepatocellular Carcinoma: Case Report and Literature Review
