Clin Endosc.
2015 Nov;48(6):576-578. 10.5946/ce.2015.48.6.576.
Successful Palliation of a Malignant Cologastric Fistula with a Covered Self-Expanding Metal Stent
- Affiliations
-
- 1Department of Surgical Gastroenterology, Aarhus University Hospital, Aarhus, Denmark. mathbrei@rm.dk
- KMID: 2380420
- DOI: http://doi.org/10.5946/ce.2015.48.6.576
Abstract
- When patients present with malignant cologastric fistulas, the tumor stage is often advanced and management is only palliative. We report the case of a 75-year-old man with a symptomatic cologastric fistula arising from an advanced tumor in the transverse colon, previously stented owing to malignant obstruction. An 8-cm-long covered self-expanding metal stent (COMVI enteral colonic stent; Taewoong Medical) was placed inside the primary stent, which sealed the fistula and completely alleviated the symptoms. Considering the successful outcome, we propose that insertion of a covered stent be considered in the palliative management of patients with malignant cologastric fistulas.
Keyword
Figure
-
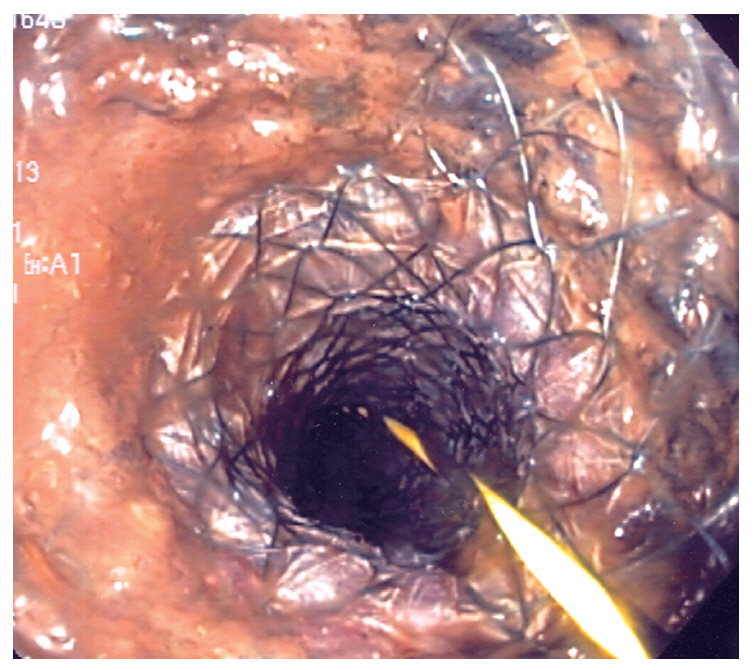
Fig. 1. Endoscopic view of the newly placed covered stent.
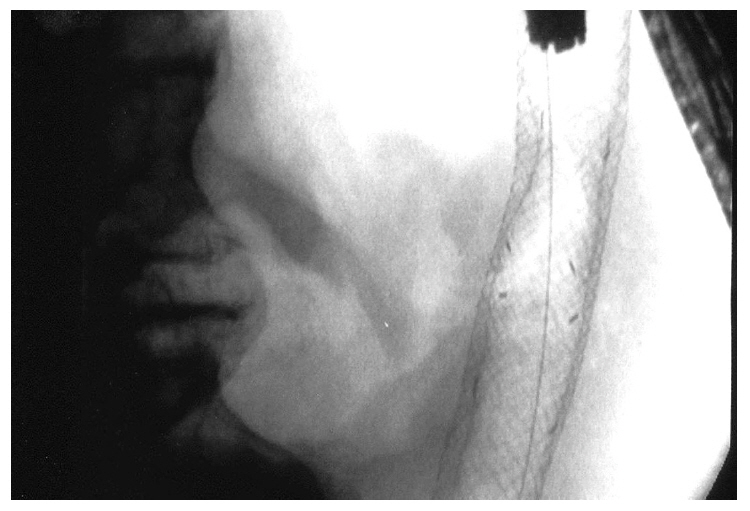
Fig. 2. Fluoroscopic image of the two stents with the colonoscope tip inside the distal end of the stents and the guidewire left in situ.
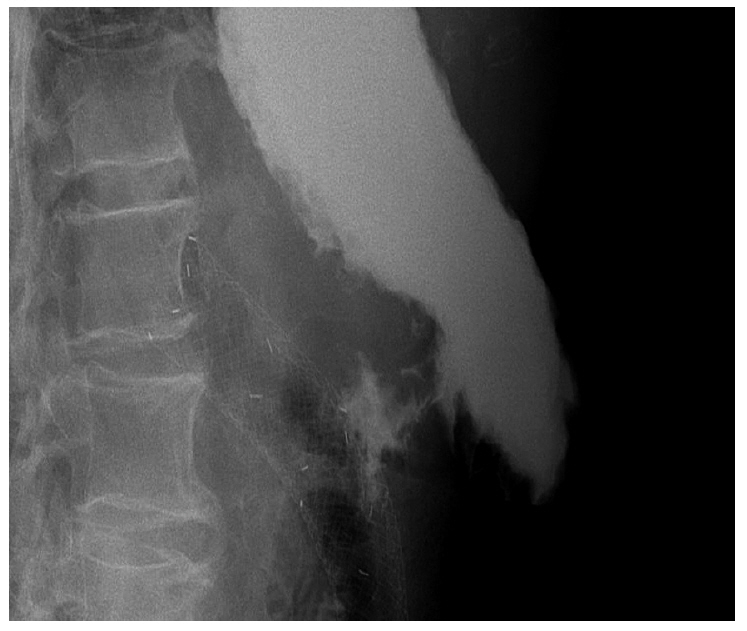
Fig. 3. Contrast study showing filling of the cologastric fistula and accumulation of contrast outside the stent with no contrast passage to the colon.
Reference
-
1. Low DE, Kozarek RA. Comparison of conventional and wire mesh expandable prostheses and surgical bypass in patients with malignant esophagorespiratory fistulas. Ann Thorac Surg. 1998; 65:919–923.
Article2. May A, Hahn EG, Ell C. Self-expanding metal stents for palliation of malignant obstruction in the upper gastrointestinal tract. Comparative assessment of three stent types implemented in 96 implantations. J Clin Gastroenterol. 1996; 22:261–266.3. Hu Y, Zhao YF, Chen LQ, et al. Comparative study of different treatments for malignant tracheoesophageal/bronchoesophageal fistulae. Dis Esophagus. 2009; 22:526–531.
Article4. Abadal JM, Echenagusia A, Simo G, Camunez F. Treatment of malignant esophagorespiratory fistulas with covered stents. Abdom Imaging. 2001; 26:565–569.
Article5. Matsuo S, Eto T, Ohara O, Miyazaki J, Tsunoda T, Kanematsu T. Gastrocolic fistula originating from transverse colon cancer: report of a case and review of the Japanese literature. Surg Today. 1994; 24:1085–1089.
Article6. Stamatakos M, Karaiskos I, Pateras I, Alexiou I, Stefanaki C, Kontzoglou K. Gastrocolic fistulae: from Haller till nowadays. Int J Surg. 2012; 10:129–133.
Article7. Forshaw MJ, Dastur JK, Murali K, Parker MC. Long-term survival from gastrocolic fistula secondary to adenocarcinoma of the transverse colon. World J Surg Oncol. 2005; 3:9.8. Casey J, Lorenzo G. Gastrocolic fistula. J Natl Med Assoc. 1986; 78:330–332.9. Marshall SF, Knud-Hansen J. Gastrojejunocolic and gastrocolic fistulas. Ann Surg. 1957; 145:770–782.
Article10. Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004; 99:2051–2057.
Article11. Shim CS, Cho JY, Jung IS, et al. Through-the-scope double colonic stenting in the management of inoperable proximal malignant colonic obstruction: a pilot study. Endoscopy. 2004; 36:426–431.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Comparative Study on the Efficacy of Covered Metal Stent and Plastic Stent in Malignant Biliary Obstruction
- Malignant Cologastric Fistula: Report of three cases
- Stepwise Algorithmic Approach to Endoscopic Removal of Biliary Partially Covered and Uncovered Self-Expanding Metal Stents (with Videos)
- A Case of Spontaneous Esophagopleural Fistula Successfully Treated by Endoscopic Stent Insertion
- Endoscopic Stent Placement in the Palliation of Malignant Biliary Obstruction
