Clin Endosc.
2015 Nov;48(6):566-569. 10.5946/ce.2015.48.6.566.
Delayed Pneumoperitoneum and Acute Pulmonary Edema Secondary to Acute Gastric Dilatation
- Affiliations
-
- 1Department of Emergency Medicine, Kyungpook National University School of Medicine, Daegu, Korea. kim7155@knu.ac.kr
- KMID: 2380418
- DOI: http://doi.org/10.5946/ce.2015.48.6.566
Abstract
- Pneumoperitoneum caused by acute gastric dilatation (AGD) is a very rare complication. We report a case of pneumoperitoneum and acute pulmonary edema caused by AGD in a patient with Parkinson's disease. A 78-year-old woman presented with pneumonia and AGD. We inserted a nasogastric tube and administered empirical antibiotics. We performed an endoscopy, and perforation or necrosis of the stomach and pyloric stenosis were not observed. Thirty-six hours after admission, the patient suddenly developed dyspnea and shock, and eventually died. We suspected the cause of death was pneumoperitoneum and acute pulmonary edema caused by AGD during the conservative treatment period. Immunocompromised patients with chronic illness require close observation even if they do not show any symptoms suggestive of complications. Even if the initial endoscopic or abdominal radiologic findings do not show gastric necrosis or perforation, follow-up with endoscopy is essential to recognize complications of AGD early.
MeSH Terms
Figure
-
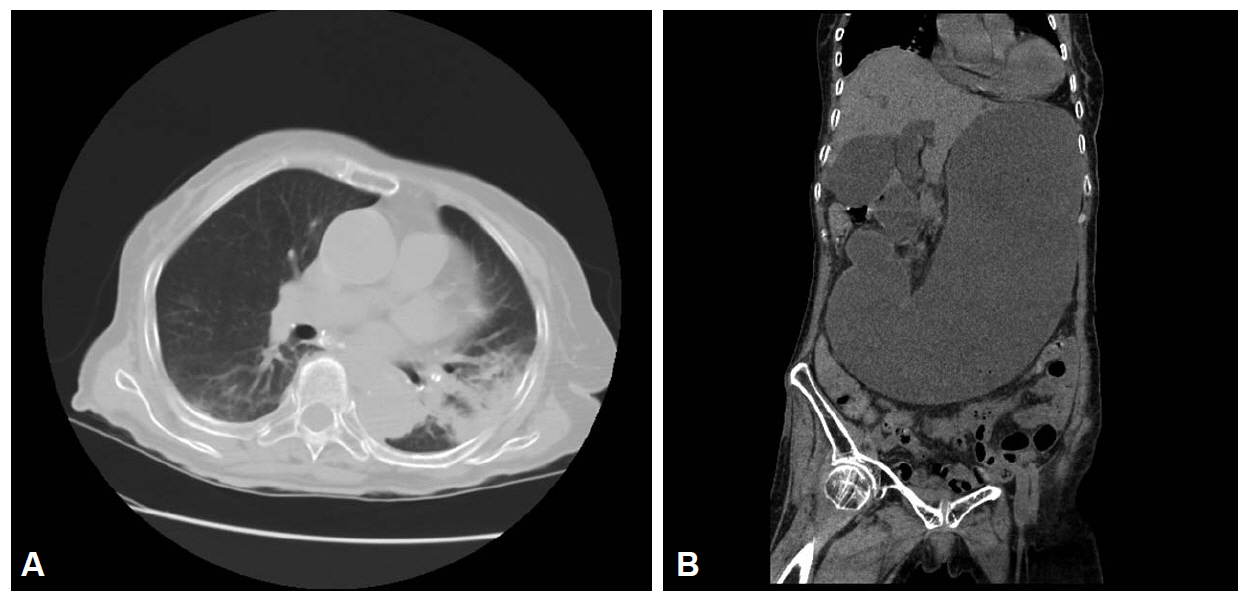
Fig. 1. Noncontrast computed tomography scan of the patient. (A) Pneumonic consolidation is seen in the left lower lobe of the lung. (B) Abdominal computed tomography scan showing a severely dilated stomach with fluid retention and absence of free air in the abdomen.
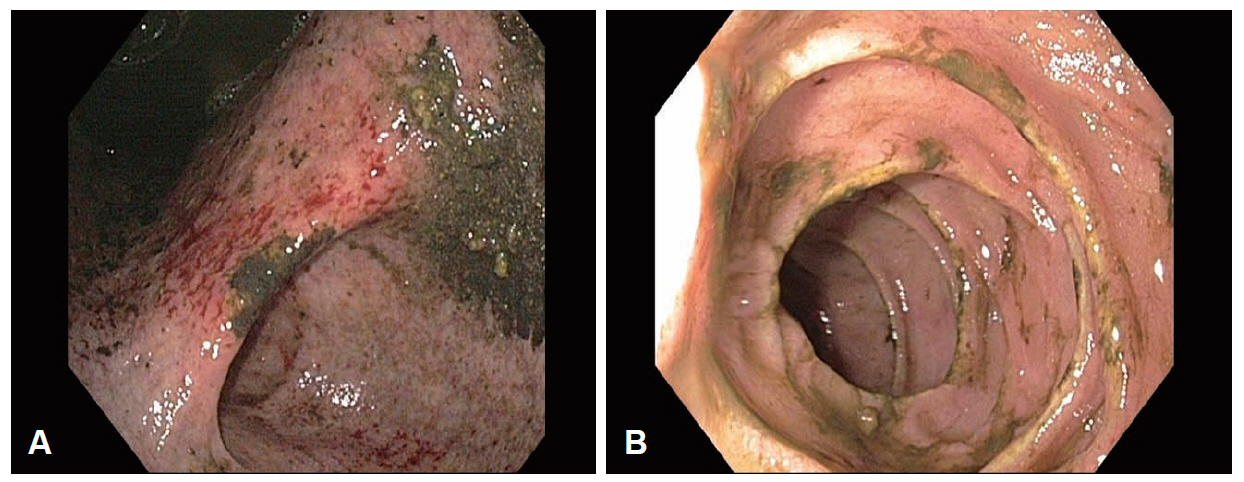
Fig. 2. Esophagogastroduodenoscopic images. (A) There is a large volume of remnant food and liquid materials and multiple superficial ulcers and erosions over the entire wall of the stomach. (B) No evidence of duodenal ulcer or pyloric obstruction is visible.
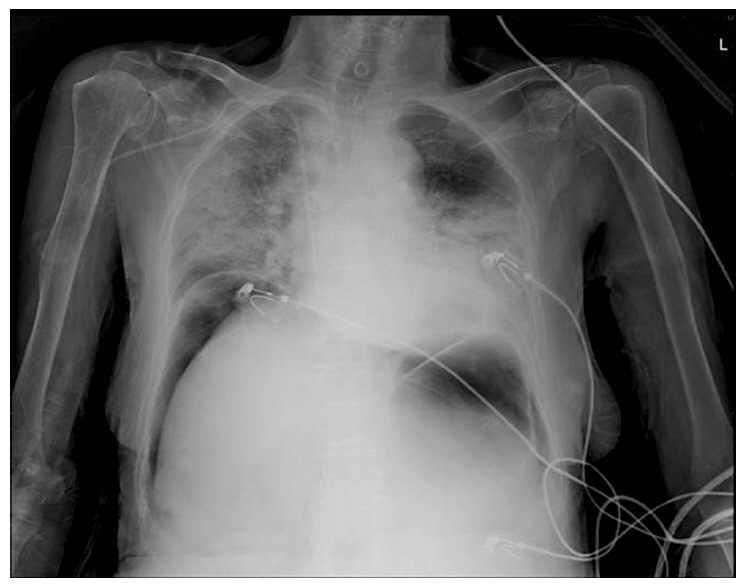
Fig. 3. Radiograph at 36 hours follow-up. The image shows the pneumoperitoneum and increased infiltration in both lung fields.
Reference
-
1. Cox A, Marks DJ. Acute gastric dilatation causing respiratory distress. JRSM Short Rep. 2011; 2:41.
Article2. Luncă S, Rikkers A, Stănescu A. Acute massive gastric dilatation: severe ischemia and gastric necrosis without perforation. Rom J Gastroenterol. 2005; 14:279–283.3. Cogbill TH, Bintz M, Johnson JA, Strutt PJ. Acute gastric dilatation after trauma. J Trauma. 1987; 27:1113–1117.
Article4. Adson DE, Mitchell JE, Trenkner SW. The superior mesenteric artery syndrome and acute gastric dilatation in eating disorders: a report of two cases and a review of the literature. Int J Eat Disord. 1997; 21:103–114.
Article5. Todd SR, Marshall GT, Tyroch AH. Acute gastric dilatation revisited. Am Surg. 2000; 66:709–710.6. Turan M, Sen M, Canbay E, Karadayi K, Yildiz E. Gastric necrosis and perforation caused by acute gastric dilatation: report of a case. Surg Today. 2003; 33:302–304.7. Abdu RA, Garritano D, Culver O. Acute gastric necrosis in anorexia nervosa and bulimia. Two case reports. Arch Surg. 1987; 122:830–832.8. Nagai T, Yokoo M, Tomizawa T, Mori M. Acute gastric dilatation accompanied by diabetes mellitus. Intern Med. 2001; 40:320–323.
Article9. Backett SA. Acute pancreatitis and gastric dilatation in a patient with anorexia nervosa. Postgrad Med J. 1985; 61:39–40.
Article10. Edlich RF, Borner JW, Kuphal J, Wangensteen OH. Gastric blood flow. I. Its distribution during gastric distention. Am J Surg. 1970; 120:35–37.11. Kerstein MD, Goldberg B, Panter B, Tilson MD, Spiro H. Gastric infarction. Gastroenterology. 1974; 67:1238–1239.
Article12. Saul SH, Dekker A, Watson CG. Acute gastric dilatation with infarction and perforation. Report of fatal outcome in patient with anorexia nervosa. Gut. 1981; 22:978–983.
Article13. Chaun H. Massive gastric dilatation of uncertain etiology. Can Med Assoc J. 1969; 100:346–348.14. Gyurkovics E, Tihanyi B, Szijarto A, et al. Fatal outcome from extreme acute gastric dilation after an eating binge. Int J Eat Disord. 2006; 39:602–605.
Article15. Holtkamp K, Mogharrebi R, Hanisch C, Schumpelick V, Herpertz-Dahlmann B. Gastric dilatation in a girl with former obesity and atypical anorexia nervosa. Int J Eat Disord. 2002; 32:372–376.
Article16. Lim JE, Duke GL, Eachempati SR. Superior mesenteric artery syndrome presenting with acute massive gastric dilatation, gastric wall pneumatosis, and portal venous gas. Surgery. 2003; 134:840–843.
Article17. Mishima T, Kohara N, Tajima Y, et al. Gastric rupture with necrosis following acute gastric dilatation: report of a case. Surg Today. 2012; 42:997–1000.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Pulmonary Edema after Coil Embolization in a Patient with Subarachnoid Hemorrhage: A Case Report
- Pulmonary Edema secondary to aryngospasm after Extubation
- Noncadiogenic Pulmonary Edema Following Upper Airway Obetruction - a case report
- Pulmonary edema in acute carbon monoxide poisoning
- Acute Pulmonary Edema Following Esophagoscopy - A case report
