Endoluminal Closure of Colon Perforation with Endoscopic Band Ligation: Technical Feasibility and Safety in an In Vivo Canine Model
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University College of Medicine, Cheongju, Korea.
- 2Department of Veterinary Surgery, Chungbuk National University College of Veterinary Medicine, Cheongju, Korea.
- 3Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. thlee9@schmc.ac.kr
- 4Department of Biomedical Engineering, Chungbuk National University College of Medicine, Cheongju, Korea.
- KMID: 2380412
- DOI: http://doi.org/10.5946/ce.2015.48.6.534
Abstract
- BACKGROUND/AIMS
Endoscopic band ligation (EBL) is an accepted method in the management of variceal bleeding; however, there is little evidence on the safety and feasibility of EBL for the closure of bowel perforation. In this study, we aimed to evaluate the technical feasibility and efficacy of EBL in iatrogenic colon perforation by using a canine model.
METHODS
We established an iatrogenic colon perforation model by using seven beagle dogs. Longitudinal 1.5- to 1.7-cm colon perforations were created with a needle knife and an insulated-tip knife, and the perforation was subsequently closed with EBL. During a 2-week follow-up period, the animals were carefully monitored and then euthanized for pathologic examination.
RESULTS
The EBL of iatrogenic colon perforations was successful in all dogs. The mean procedure time for EBL closure with one to three bands was 191.7 seconds, and there were no immediate complications. One animal was euthanized after 3 days because of peritonitis. There were no clinical and laboratory features of sepsis or peritonitis in the remaining six animals. On necropsy, we did not find any fecal peritonitis, pericolonic abscess formation, or transmural dehiscence at the perforation site. Histopathology demonstrated inflamed granulation tissue and scar lesions replaced by fibrosis.
CONCLUSIONS
EBL might be a feasible and safe method for the management of iatrogenic colon perforations in an in vivo model.
MeSH Terms
Figure
-
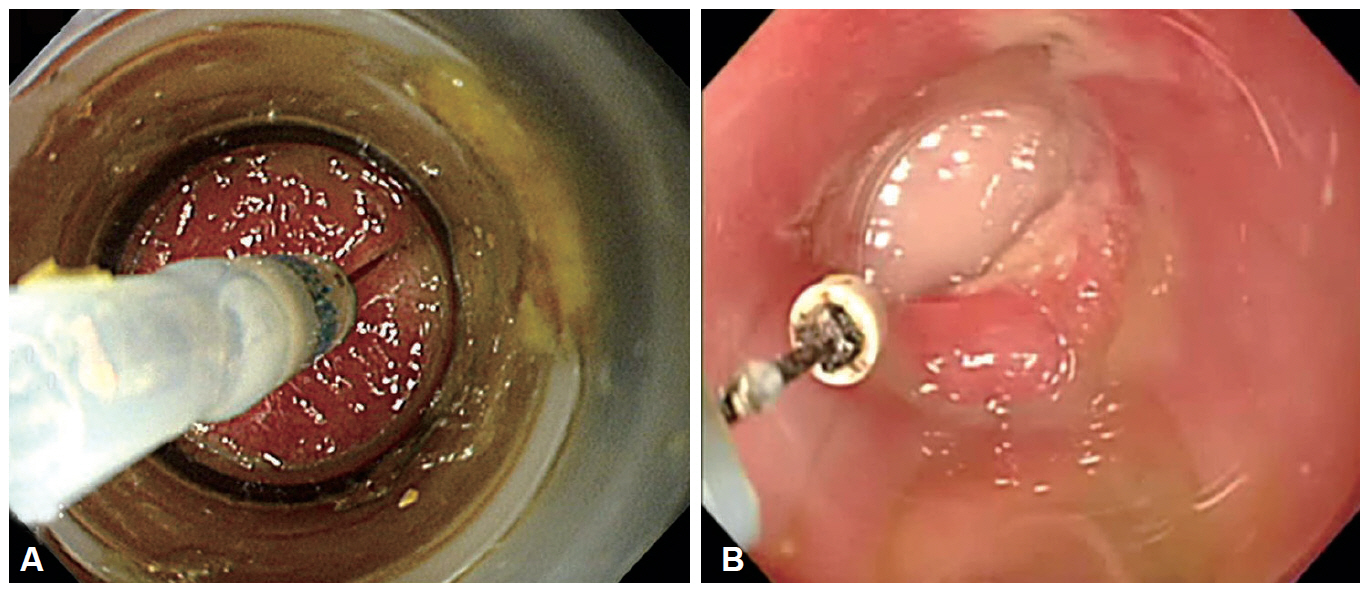
Fig. 1. An iatrogenic 1.5-cm colon perforation model. (A) A small perforation is made with a needle knife, and (B) is widened longitudinally by using an insulated-tip knife until the cap-fitted endoscope could easily pass into the peritoneal cavity.

Fig. 2. (A) A full-thickness incision is made with an endoscopic knife to the colon in the iatrogenic model. (B) Endoscopic band ligation is used to make a mushroom-like banded mucosa to complete the closure. (C) A band ligates the perforation hole incompletely, although it reduces the size of the hole in a zipper-like fashion. (D) Additional band ligation closes the perforation completely.
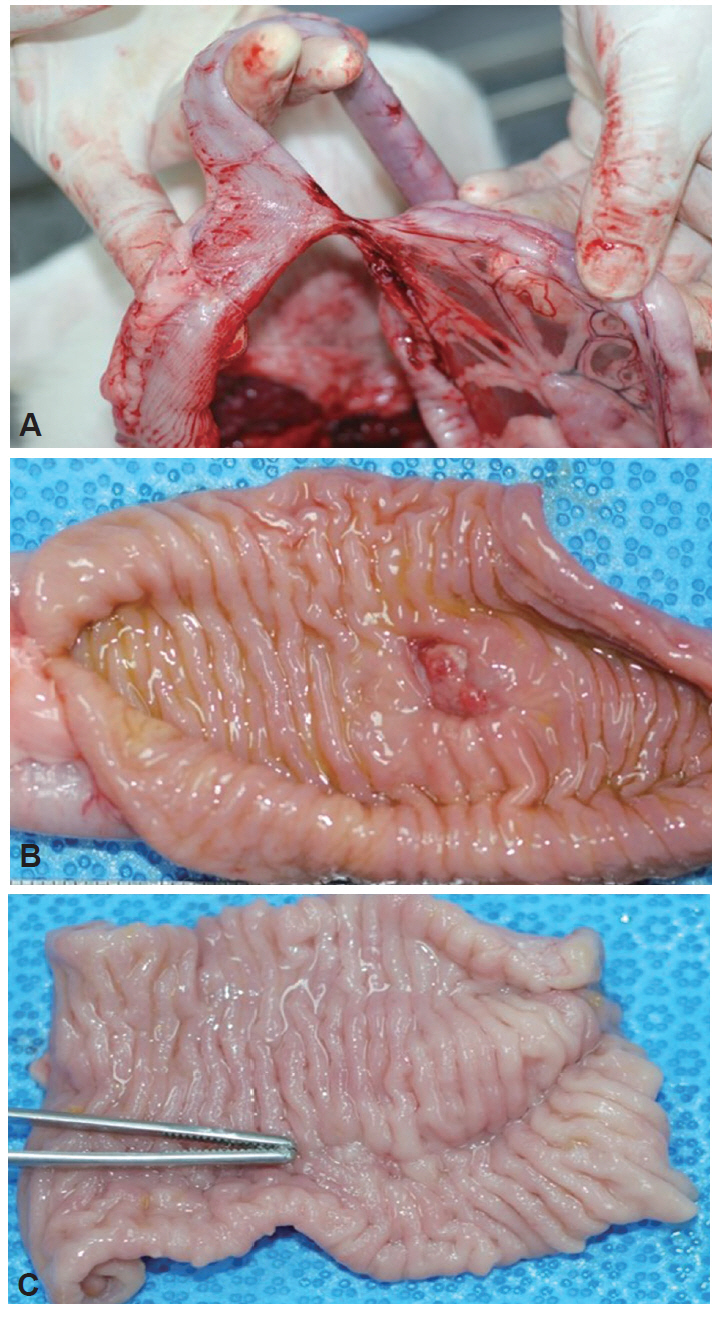
Fig. 3. Macroscopic view of a necropsy. (A) An external view of the perforation site shows local adhesion with a fibrous band and distant adhesion with the small bowel. (B) An internal view of the perforation site shows an ulcer at the healing stage and (C) a completely healed scar.

Fig. 4. Microscopic finding of the healed site of endoscopic band ligation. (A) Complete reepithelialization of the mucosa is seen (arrow). Inflamed granulation tissue remains in the submucosa and serosa (arrowheads) (H&E stain, ×10). (B) Defects of the muscularis propria (arrowheads indicate preexisting smooth muscle bundles) are replaced by fibrosis (arrows) (H&E stain, ×10). (C) The fibrotic adhesion with the small bowel is seen at the site of healing of the perforation on the serosal surface (H&E stain, ×1). (D) Severe fibrosis with chronic inflammation is observed in the pericolic fat tissue (H&E stain, ×40).
Reference
-
1. Lee TH, Bang BW, Jeong JI, et al. Primary endoscopic approximation suture under cap-assisted endoscopy of an ERCP-induced duodenal perforation. World J Gastroenterol. 2010; 16:2305–2310.
Article2. Baron TH, Wong Kee Song LM, Zielinski MD, Emura F, Fotoohi M, Kozarek RA. A comprehensive approach to the management of acute endoscopic perforations (with videos). Gastrointest Endosc. 2012; 76:838–859.
Article3. Kim JS, Kim BW, Kim JI, et al. Endoscopic clip closure versus surgery for the treatment of iatrogenic colon perforations developed during diagnostic colonoscopy: a review of 115,285 patients. Surg Endosc. 2013; 27:501–504.
Article4. Mangiavillano B, Viaggi P, Masci E. Endoscopic closure of acute iatrogenic perforations during diagnostic and therapeutic endoscopy in the gastrointestinal tract using metallic clips: a literature review. J Dig Dis. 2010; 11:12–18.
Article5. Panteris V, Haringsma J, Kuipers EJ. Colonoscopy perforation rate, mechanisms and outcome: from diagnostic to therapeutic colonoscopy. Endoscopy. 2009; 41:941–951.
Article6. Matthes K, Jung Y, Kato M, Gromski MA, Chuttani R. Efficacy of full-thickness GI perforation closure with a novel over-the-scope clip application device: an animal study. Gastrointest Endosc. 2011; 74:1369–1375.
Article7. Yang DH, Byeon JS, Lee KH, et al. Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopy-associated bowel perforation? Surg Endosc. 2010; 24:1177–1185.
Article8. Kirschniak A, Subotova N, Zieker D, Königsrainer A, Kratt T. The Over-The-Scope Clip (OTSC) for the treatment of gastrointestinal bleeding, perforations, and fistulas. Surg Endosc. 2011; 25:2901–2905.
Article9. Van Stiegmann G, Goff JS. Endoscopic esophageal varix ligation: preliminary clinical experience. Gastrointest Endosc. 1988; 34:113–117.
Article10. Brown GR, Harford WV, Jones WF. Endoscopic band ligation of an actively bleeding Dieulafoy lesion. Gastrointest Endosc. 1994; 40:501–503.
Article11. Slivka A, Parsons WG, Carr-Locke DL. Endoscopic band ligation for treatment of post-polypectomy hemorrhage. Gastrointest Endosc. 1994; 40(2 Pt 1):230–232.
Article12. Fan CS, Soon MS. Repair of a polypectomy-induced duodenal perforation with a combination of hemoclip and band ligation. Gastrointest Endosc. 2007; 66:203–205.
Article13. Lee HN, Kim EJ, Park SK, et al. A case of a successful band ligation of a colonic perforation during diagnostic colonoscopy. Korean J Gastrointest Endosc. 2010; 41:176–179.14. Moon SY, Park CH, Yoon SM, et al. Repair of an endoscopic submucosal dissection-induced rectal perforation with band ligation. Gastrointest Endosc. 2009; 69:160–161.
Article15. Han JH, Park S, Youn S. Endoscopic closure of colon perforation with band ligation; salvage technique after endoclip failure. Clin Gastroenterol Hepatol. 2011; 9:e54–e55.
Article16. Han JH, Lee TH, Jung Y, et al. Rescue endoscopic band ligation of iatrogenic gastric perforations following failed endoclip closure. World J Gastroenterol. 2013; 19:955–959.
Article17. Lee TH, Han JH, Jung Y, et al. Comparison of endoscopic band ligation and endoclip closure of colonic perforation: technical feasibility and efficacy in an ex vivo pig model. Dig Endosc. 2014; 26:659–664.18. Culp WT, Zeldis TE, Reese MS, Drobatz KJ. Primary bacterial peritonitis in dogs and cats: 24 cases (1990-2006). J Am Vet Med Assoc. 2009; 234:906–913.
Article19. Hurlstone DP, Sanders DS, Cross SS, et al. Colonoscopic resection of lateral spreading tumours: a prospective analysis of endoscopic mucosal resection. Gut. 2004; 53:1334–1339.
Article20. Tanaka S, Haruma K, Oka S, et al. Clinicopathologic features and endoscopic treatment of superficially spreading colorectal neoplasms larger than 20 mm. Gastrointest Endosc. 2001; 54:62–66.
Article21. Brooker JC, Saunders BP, Shah SG, Williams CB. Endoscopic resection of large sessile colonic polyps by specialist and non-specialist endoscopists. Br J Surg. 2002; 89:1020–1024.
Article22. Fujii T, Ono A, Fu KI. A novel endoscopic suturing technique using a specially designed so-called “8-ring” in combination with resolution clips (with videos). Gastrointest Endosc. 2007; 66:1215–1220.
Article23. Ryou M, Fong DG, Pai RD, Sauer J, Thompson CC. Evaluation of a novel access and closure device for NOTES applications: a transcolonic survival study in the porcine model (with video). Gastrointest Endosc. 2008; 67:964–969.
Article24. Farrell JJ, Graeme-Cook F, Kelsey PB. Treatment of bleeding colonic diverticula by endoscopic band ligation: an in-vivo and ex-vivo pilot study. Endoscopy. 2003; 35:823–829.
Article25. Setoyama T, Ishii N, Fujita Y. Enodoscopic band ligation (EBL) is superior to endoscopic clipping for the treatment of colonic diverticular hemorrhage. Surg Endosc. 2011; 25:3574–3578.
Article26. Ishii N, Setoyama T, Deshpande GA, et al. Endoscopic band ligation for colonic diverticular hemorrhage. Gastrointest Endosc. 2012; 75:382–387.
Article27. Zepeda-Gómez S, Marcon NE. Endoscopic band ligation for nonvariceal bleeding: a review. Can J Gastroenterol. 2008; 22:748–752.
Article28. Ahn DW, Lee SH, Park YS, et al. Hemostatic efficacy and clinical outcome of endoscopic treatment of Dieulafoy’s lesions: comparison of endoscopic hemoclip placement and endoscopic band ligation. Gastrointest Endosc. 2012; 75:32–38.
Article29. Angsuwatcharakon P, Thienchanachaiya P, Pantongrag-Brown L, Rerknimitr R. Endoscopic band ligation to create an omental patch for closure of a colonic perforation. Endoscopy. 2012; 44 Suppl 2 UCTN:E90–E91.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Repair of an Endoscopic Retrograde Cholangiopancreatography-Related Large Duodenal Perforation Using Double Endoscopic Band Ligation and Endoclipping
- Endoscopic Mucosal Resection with Band Ligation for Two Cases of Gastric Flat Adenoma
- Results of Experimental Canine Gastric Wall Ligation using 0-shaped Rubber Band
- A Case of a Successful Band Ligation of a Colonic Perforation during Diagnostic Colonoscopy
- Recent Advanced Endoscopic Management of Endoscopic Retrograde Cholangiopancreatography Related Duodenal Perforations
