Long-Term Survival after T-cell Lymphoblastic Lymphoma Treated with One Cycle of Hyper-CVAD Regimen
- Affiliations
-
- 1Department of Internal Medicine, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea. cis@eulji.ac.kr
- 2Department of Pathology, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 2380397
- DOI: http://doi.org/10.4143/crt.2013.122
Abstract
- T-lymphoblastic lymphoma (T-LBL) is a rare form of aggressive non-Hodgkin's lymphoma. The standard approach for management of T-LBL involves intensive multiagent chemotherapy regimens for induction and consolidation phases with central nervous system prophylaxis and a maintenance phase lasting 12-18 months. We report on a case of long-term survival after one cycle of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD) and high-dose methotrexate. A 30-year-old woman diagnosed with T-LBL with a large mediastinal mass underwent one cycle of hyper-CVAD. Four days after the start of treatment, the mediastinal mass was markedly reduced. Treatment continued with one cycle of consolidation chemotherapy, comprising high-dose methotrexate and high-dose cytarabine. The patient then refused all further chemotherapeutic treatment. Seven years have passed without relapse.
MeSH Terms
-
Adult
Central Nervous System
Consolidation Chemotherapy
Cyclophosphamide
Cytarabine
Dexamethasone
Doxorubicin
Drug Therapy
Female
Humans
Lymphoma
Lymphoma, Non-Hodgkin
Methotrexate
Precursor Cell Lymphoblastic Leukemia-Lymphoma*
Precursor T-Cell Lymphoblastic Leukemia-Lymphoma
Recurrence
Remission Induction
T-Lymphocytes*
Vincristine
Cyclophosphamide
Cytarabine
Dexamethasone
Doxorubicin
Methotrexate
Vincristine
Figure
-
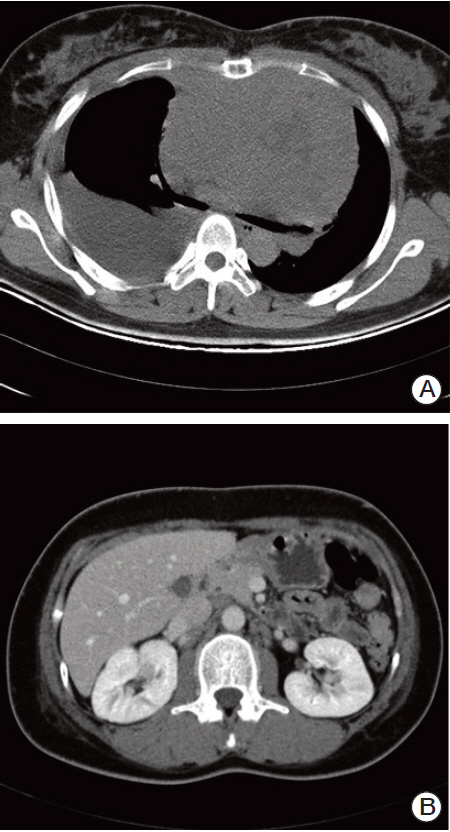
Fig. 1. Computed tomography (CT) at initial diagnosis. (A) Chest CT scan showed a large mediastinal mass, pleural effusion. (B) Abdominal CT scan showed left para-aortic lymphadenopathy.
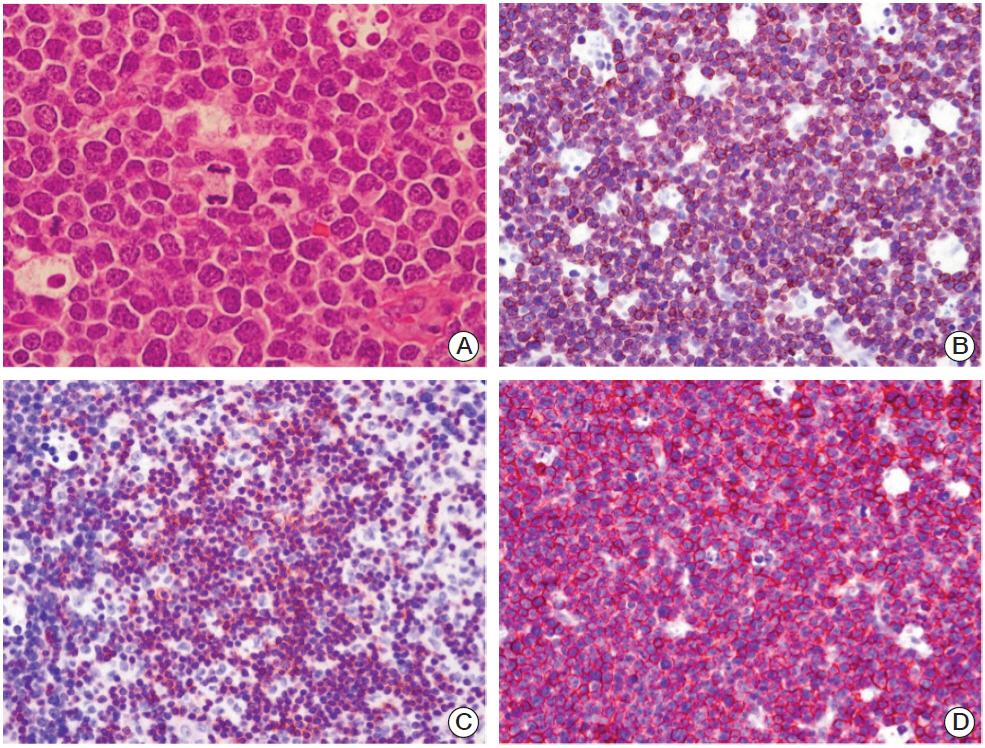
Fig. 2. Microscopic findings of the precursor T-cell lymphoblastic lymphoma from the axillary lymph node. (A) Most tumor cells show immature nuclei with fine chromatin, convoluted nuclear contours, and frequent mitotic figures (H&E staining, ×1,000). On immunohistochemical staining, tumor cells were positive for CD3 (B) CD5 (C), and CD99 (D) (B-D, ×400).

Fig. 3. Comparison of chest X-ray. (A) Before treatment of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (hyper-CVAD), on April 3, 2006. (B) Chest X-ray showed that the mediastinal mass had decreased after performance of hyper-CAVD, on April 7, 2006.
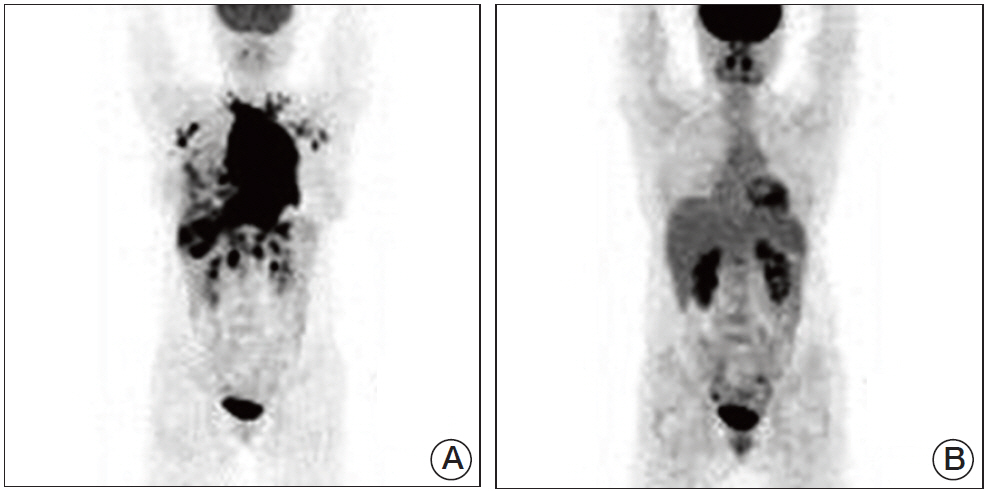
Fig. 4. Comparison of position emission tomography-computed tomography (PET-CT), before and after treatment. (A) In March 2006, PET-CT showed the hypermetabolic mediastinal mass with multiple lymphadenopathy and pleural invasion. (B) In November 2006, after chemotherapy, PET-CT showed no hypermetabolic lesion.
Reference
-
References
1. A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin’s lymphoma. The Non-Hodgkin’s Lymphoma Classification Project. Blood. 1997; 89:3909–18.2. Portell CA, Sweetenham JW. Adult lymphoblastic lymphoma. Cancer J. 2012; 18:432–8.
Article3. Sweetenham JW. Treatment of lymphoblastic lymphoma in adults. Oncology (Williston Park). 2009; 23:1015–20.4. Hoelzer D, Gokbuget N. T-cell lymphoblastic lymphoma and T-cell acute lymphoblastic leukemia: a separate entity? Clin Lymphoma Myeloma. 2009; 9 Suppl 3:S214–21.
Article5. Raetz EA, Perkins SL, Bhojwani D, Smock K, Philip M, Carroll WL, et al. Gene expression profiling reveals intrinsic differences between T-cell acute lymphoblastic leukemia and T-cell lymphoblastic lymphoma. Pediatr Blood Cancer. 2006; 47:130–40.
Article6. Uyttebroeck A, Suciu S, Laureys G, Robert A, Pacquement H, Ferster A, et al. Treatment of childhood T-cell lymphoblastic lymphoma according to the strategy for acute lymphoblastic leukaemia, without radiotherapy: long term results of the EORTC CLG 58881 trial. Eur J Cancer. 2008; 44:840–6.
Article7. Jabbour E, Koscielny S, Sebban C, Peslin N, Patte C, Gargi T, et al. High survival rate with the LMT-89 regimen in lymphoblastic lymphoma (LL), but not in T-cell acute lymphoblastic leukemia (T-ALL). Leukemia. 2006; 20:814–9.
Article8. Cortelazzo S, Ponzoni M, Ferreri AJ, Hoelzer D. Lymphoblastic lymphoma. Crit Rev Oncol Hematol. 2011; 79:330–43.
Article9. Thomas DA, O'Brien S, Cortes J, Giles FJ, Faderl S, Verstovsek S, et al. Outcome with the hyper-CVAD regimens in lymphoblastic lymphoma. Blood. 2004; 104:1624–30.
Article10. Hoelzer D, Gokbuget N. Treatment of lymphoblastic lymphoma in adults. Best Pract Res Clin Haematol. 2002; 15:713–28.
Article11. Bouabdallah R, Xerri L, Bardou VJ, Stoppa AM, Blaise D, Sainty D, et al. Role of induction chemotherapy and bone marrow transplantation in adult lymphoblastic lymphoma: a report on 62 patients from a single center. Ann Oncol. 1998; 9:619–25.
Article12. Ceesay MM, Vadher B, Tinwell B, Goderya R, Sawicka E. Spontaneous remission of T lymphoblastic lymphoma. J Clin Pathol. 2008; 61:955–7.
Article13. Reiter A, Schrappe M, Ludwig WD, Tiemann M, Parwaresch R, Zimmermann M, et al. Intensive ALL-type therapy without local radiotherapy provides a 90% event-free survival for children with T-cell lymphoblastic lymphoma: a BFM group report. Blood. 2000; 95:416–21.14. Coleman CN, Picozzi VJ Jr, Cox RS, McWhirter K, Weiss LM, Cohen JR, et al. Treatment of lymphoblastic lymphoma in adults. J Clin Oncol. 1986; 4:1628–37.
Article15. Hoelzer D, Gokbuget N, Digel W, Faak T, Kneba M, Reutzel R, et al. Outcome of adult patients with T-lymphoblastic lymphoma treated according to protocols for acute lymphoblastic leukemia. Blood. 2002; 99:4379–85.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Mantle Cell Lymphoma Treated with Autologous Stem Cell Transplantation and Rituximab
- Nine-Year Survival of Lymphoblastic Lymphoma Patients
- Treatment Outcomes of Rituximab Plus Hyper-CVAD in Korean Patients with Sporadic Burkitt or Burkitt-like Lymphoma: Results of a Multicenter Analysis
- A Case of Non-T,Non-B Primary Cutaneous Lymphoblastic Lymphoma
- Long-term treatment outcomes of children and adolescents with lymphoblastic lymphoma treated with various regimens:a single-center analysis
