J Menopausal Med.
2016 Dec;22(3):184-187. 10.6118/jmm.2016.22.3.184.
Non-puerperal Uterine Inversion Presented with Hypovolemic Shock
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. yjna@pusan.ac.kr
- KMID: 2378240
- DOI: http://doi.org/10.6118/jmm.2016.22.3.184
Abstract
- We report a non-puerperal uterine inversion with nulliparous women caused by huge pedunculated submucosal fibroid. Massive bleeding from protruding mass through vagina brought the heart to stop in 42-year-old nulliparous woman. She became cardiopulmonary resuscitation survivor in emergency room and then underwent laparotomy which ended in successful myomectomy rather than hysterectomy considering her demand for future fertility. Meticulous and adequate fluid therapy and transfusion was also administered to recover from hypovolemic status. Pathologic report confirmed benign submucosal fibroid with degeneration, necrosis and abscess formation. Thus, clinician should be aware of uterine inversion when encountered with huge protruding vaginal mass and consider uterus-preserving management as surgical option when the future fertility is concerned.
Keyword
MeSH Terms
Figure
-

Fig. 1 Coronal plane on contrast enhanced computed tomography (CT) revealed the prolapsed mass in the uterus and retraction of fundus. (B) Axial plain on contrast enhanced CT revealed extravasation of contrast media (arrow), suggestive of active bleeding from the mass in the uterus.
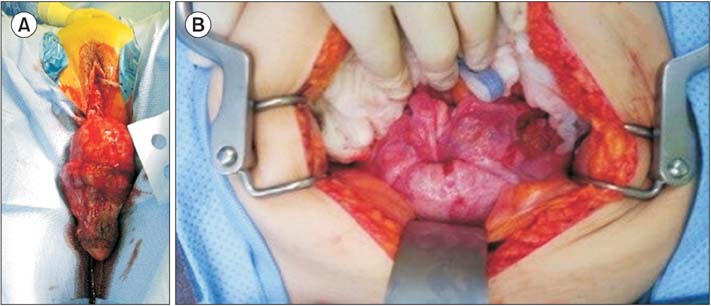
Fig. 2 Pre- and intra-operative images. (A) Huge necrotic mass protruding from the vaginal introitus. (B) The uterus is fully inverted and the fundus is not visualized in intra-operative finding.

Fig. 3 Gross finding of resected intrauterine mass in size of 22 × 11.5 × 5.8 cm. Pathologic report revealed benign leiomyoma.
Reference
-
1. Eigbefoh JO, Okogbenin SA, Omorogbe F, Mabayoje PS. Chronic uterine inversion secondary to submucous fibroid: a case report. Niger J Clin Pract. 2009; 12:106–107.2. Rathod S, Samal SK, Pallavee P, Ghose S. Non puerperal uterine inversion in a young female- a case report. J Clin Diagn Res. 2014; 8:OD01–OD02.3. Kulkarni KK, Ajmera SK. A rare case of non-puerperal acute uterine inversion. J Obstet Gynaecol India. 2014; 64:364–365.4. Lupovitch A, England ER, Chen R. Non-puerperal uterine inversion in association with uterine sarcoma: case report in a 26-year-old and review of the literature. Gynecol Oncol. 2005; 97:938–941.5. Krenning RA. Nonpuerperal uterine inversion. Review of literature. Clin Exp Obstet Gynecol. 1982; 9:12–15.6. Mihmanli V, Kilic F, Pul S, Kilinc A, Kilickaya A. Magnetic resonance imaging of non-puerperal complete uterine inversion. Iran J Radiol. 2015; 12:e9878.7. Simms-Stewart D, Frederick S, Fletcher H, Char G, Mitchell S. Postmenopausal uterine inversion treated by subtotal hysterectomy. J Obstet Gynaecol. 2008; 28:116–117.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Uterine Artery Embolization as an Effective Management and Diagnostic Tool for Puerperal Uterine Inversion with Severe Postpartum Bleeding: A Case Report
- Pelvic organ prolapse and uterine inversion: A case report and literature review
- Replacement of Uterine Inversion by the Induction of General Anesthesia: A case report
- Spontaneous Restoration of Unrecognized Uterine Inversion
- A case of uterine inversion resulted from prolapse of huge pedunculated uterine submucosal leiomyoma
