Diverse Phenotypic Expression of Cardiomyopathies in a Family with TNNI3 p.Arg145Trp Mutation
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. dukkyung.kim@gmail.com
- 2Department of Laboratory Medicine, Korea University College of Medicine, Seoul, Korea.
- 3Department of Laboratory Medicine, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Laboratory Medicine and Genetics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2377469
- DOI: http://doi.org/10.4070/kcj.2016.0213
Abstract
- Genetic diagnosis of cardiomyopathies is challenging, due to the marked genetic and allelic heterogeneity and the lack of knowledge of the mutations that lead to clinical phenotypes. Here, we present the case of a large family, in which a single TNNI3 mutation caused variable phenotypic expression, ranging from restrictive cardiomyopathy (RCMP) to hypertrophic cardiomyopathy (HCMP) to near-normal phenotype. The proband was a 57-year-old female with HCMP. Examining the family history revealed that her elder sister had expired due to severe RCMP. Using a next-generation sequencing-based gene panel to analyze the proband, we identified a known TNNI3 gene mutation, c.433C>T, which is predicted to cause an amino acid substitution (p.Arg145Trp) in the highly conserved inhibitory region of the cardiac troponin I protein. Sanger sequencing confirmed that six relatives with RCMP or near-normal phenotypes also carried this mutation. To our knowledge, this is the first genetically confirmed family with diverse phenotypic expression of cardiomyopathies in Korea. Our findings demonstrate familial implications, where a single mutation in a sarcomere protein can cause diverse phenotypic expression of cardiomyopathies.
Keyword
MeSH Terms
Figure
-

Fig. 1 Family affected by the c.433C>T (p.Arg145Trp) TNNI3 mutation. A black or gray symbol indicates clinically affected family members (gray: no symptoms or only mild heart problems). A diagonal line represents deceased family members, a question mark shows family members with unknown phenotypes, and the arrow indicates the index patient (“P”). A plus sign indicates the presence of a mutation, whereas minus sign indicates the absence of mutation. The age at death (“d”) is shown in years. Decade of the deceased age is shown as “s”. SCD: sudden cardiac death, RCMP: restrictive cardiomyopathy, HCMP: hypertrophic cardiomyopathy.
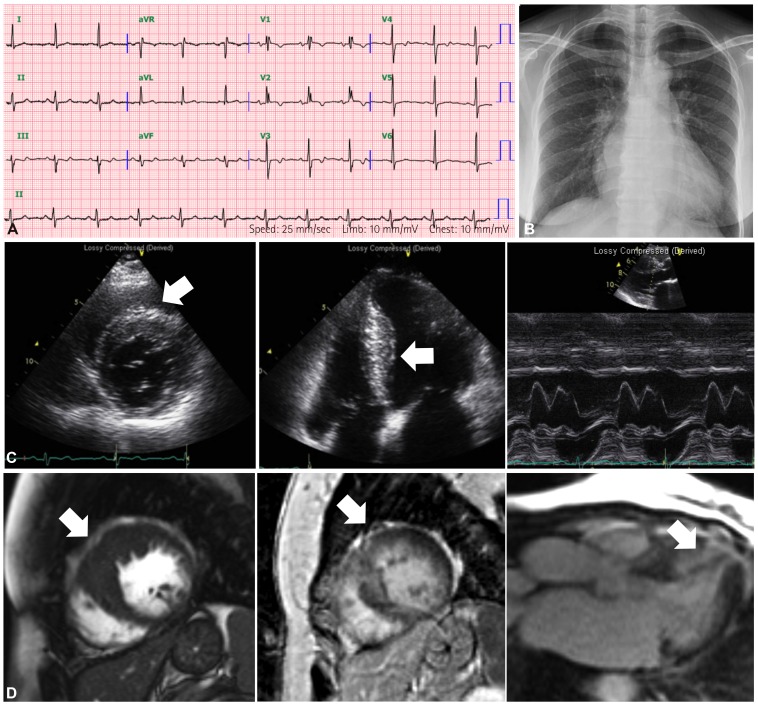
Fig. 2 Imaging findings of proband (III:4) as a 57-year-old woman. (A) Incomplete RBBB, non-specific ST-T change and regular sinus rhythm were seen on initial ECG. (B) Slight cardiomegaly (cardiothoracic ratio was 0.62) without pulmonary edema was detected on chest radiographs. (C) In the echocardiographic examination, the upper two panels showed increased thickness of the interventricular septum to a maximum of 20 mm (white arrows), consistent with HCMP. However, there was no systolic anterior motion of the mitral valve (lower panel). (D) Cine short axis view using a balanced steady-state free precession sequence revealed thickening of the apical septal and anterior wall of the left ventricle (white arrow in the first panel). Delayed enhancement images using the Turbo-FLASH sequence showed hyper-enhancement in the same area (white arrow in the second and third panel). RBBB: bundle branch block, ST-T: ST-T segment, ECG: electrocardiogram, HCMP: hypertrophic cardiomyopathy.
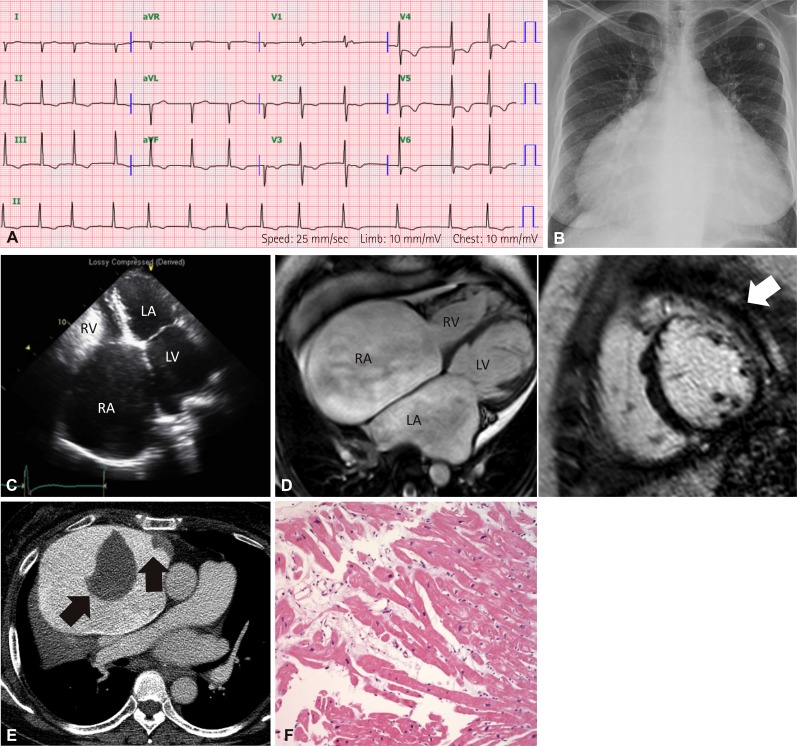
Fig. 3 Imaging findings of patient's older sister (III:2). (A) ECG showed atrial fibrillation and right ventricular hypertrophy. (B) Marked cardiomegaly was seen (cardiothoracic ratio was 0.83) in chest radiograph. (C) In echocardiographic examination, huge enlargement of both atria with preserved left ventricular systolic function was observed, consistent with RCMP. (D) Four-chamber view using balanced steady-state free precession sequence revealed marked dilatation of LA and RA without ventricular dilatation (first panel). Delayed enhancement images using Turbo-FLASH sequence showed hyperenhancement at anterior and antero-lateral wall of mid-ventricular level (white arrow). (E) Contrast-enhanced chest computed tomography demonstrated two low-attenuation and irregular-shaped masses (black arrows) in the huge right atrium, which were suspicious of thrombi. (F) Endomyocardial biopsy of the right ventricle. Myocytes showed mild focal disarray and increased nucleus size. The interstitium was widened and edematous (hematoxylin and eosin, 200×). ECG: electrocardiography, RCMP: restrictive cardiomyopathy, LA: left atrium, RA: right atrium, LV: left ventricle, RV: right ventricle.

Fig. 4 Imaging findings of the proband's mother (II:3). (A) ECG showed a mild degree of first-degree AV block and non-specific ST-T changes in inferolateral leads. (B) Cardiomegaly was not seen on chest radiograph. (C) ECG showed mild left atrial enlargement with a mild degree of diastolic dysfunction (grade 1), and normal LV wall thickness. ECG: electrocardiography, AV: atrioventricular, LA: left atrium, LV: left ventricle.
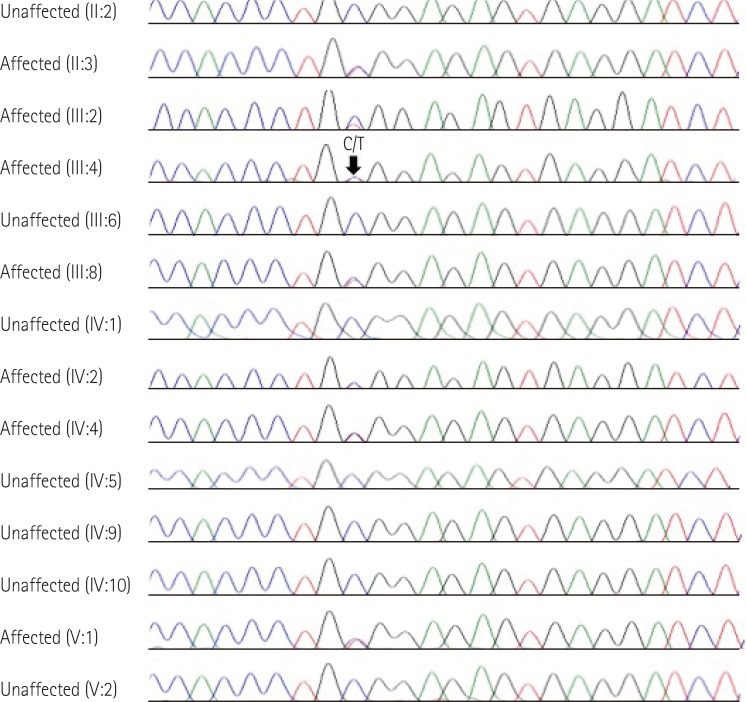
Fig. 5 Sequence analysis of the TNNI3 gene. Chromatograms show the heterozygous nonsynonymous mutation (c.433C>T, p.Arg145Trp) of the TNNI3 gene in the proband (III:4), individuals II:3, III:2, III:8, IV:2, IV:4, and V:1, and the normal sequence in individuals II:2, III:6, IV:1, IV:5, IV:9, IV:10, and V:2 (arrow).
Reference
-
1. Tariq M, Ware SM. Importance of genetic evaluation and testing in pediatric cardiomyopathy. World J Cardiol. 2014; 6:1156–1165. PMID: 25429328.2. Callis TE, Jensen BC, Weck KE, Willis MS. Evolving molecular diagnostics for familial cardiomyopathies: at the heart of it all. Expert Rev Mol Diagn. 2010; 10:329–351. PMID: 20370590.3. Roma-Rodrigues C, Fernandes AR. Genetics of hypertrophic cardiomyopathy: advances and pitfalls in molecular diagnosis and therapy. Appl Clin Genet. 2014; 7:195–208. PMID: 25328416.4. Willott RH, Gomes AV, Chang AN, Parvatiyar MS, Pinto JR, Potter JD. Mutations in Troponin that cause HCM, DCM AND RCM: what can we learn about thin filament function? J Mol Cell Cardiol. 2010; 48:882–892. PMID: 19914256.5. Luedde M, Ehlermann P, Weichenhan D, et al. Severe familial left ventricular non-compaction cardiomyopathy due to a novel troponin T (TNNT2) mutation. Cardiovasc Res. 2010; 86:452–460. PMID: 20083571.6. Mogensen J, Kubo T, Duque M, et al. Idiopathic restrictive cardiomyopathy is part of the clinical expression of cardiac troponin I mutations. J Clin Invest. 2003; 111:209–216. PMID: 12531876.7. Vallins WJ, Brand NJ, Dabhade N, Butler-Browne G, Yacoub MH, Barton PJ. Molecular cloning of human cardiac troponin I using polymerase chain reaction. FEBS Lett. 1990; 270:57–61. PMID: 2226790.8. Bhavsar PK, Brand NJ, Yacoub MH, Barton PJ. Isolation and characterization of the human cardiac troponin I gene (TNNI3). Genomics. 1996; 35:11–23. PMID: 8661099.9. Gomes AV, Liang J, Potter JD. Mutations in human cardiac troponin I that are associated with restrictive cardiomyopathy affect basal ATPase activity and the calcium sensitivity of force development. J Biol Chem. 2005; 280:30909–30915. PMID: 15961398.10. Kobayashi T, Solaro RJ. Increased Ca2+ affinity of cardiac thin filaments reconstituted with cardiomyopathy-related mutant cardiac troponin I. J Biol Chem. 2006; 281:13471–13477. PMID: 16531415.11. Davis J, Wen H, Edwards T, Metzger JM. Allele and species dependent contractile defects by restrictive and hypertrophic cardiomyopathy-linked troponin I mutants. J Mol Cell Cardiol. 2008; 44:891–904. PMID: 18423659.12. Perry SV. Troponin I: inhibitor or facilitator. Mol Cell Biochem. 1999; 190:9–32. PMID: 10098965.13. Lang R, Gomes AV, Zhao J, Housmans PR, Miller T, Potter JD. Functional analysis of a troponin I (R145G) mutation associated with familial hypertrophic cardiomyopathy. J Biol Chem. 2002; 277:11670–11678. PMID: 11801593.14. Felker GM, Thompson RE, Hare JM, et al. Underlying causes and long-term survival in patients with initially unexplained cardiomyopathy. N Engl J Med. 2000; 342:1077–1084. PMID: 10760308.15. Webber SA, Lipshultz SE, Sleeper LA, et al. Outcomes of restrictive cardiomyopathy in childhood and the influence of phenotype: a report from the Pediatric Cardiomyopathy Registry. Circulation. 2012; 126:1237–1244. PMID: 22843787.16. Zou Y, Wang J, Liu X, et al. Multiple gene mutations, not the type of mutation, are the modifier of left ventricle hypertrophy in patients with hypertrophic cardiomyopathy. Mol Biol Rep. 2013; 40:3969–3976. PMID: 23283745.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiomyopathies with Mixed and Inapparent Morphological Features in Cardiac Troponin I3 Mutation
- Phenotypic Difference of CLCN1 Gene Variant (A313T) in a Korean Family with Myotonia Congenita
- Epidermal Growth Factor Receptor Expression of Non-small Cell Carcinoma and Its Relationship with Genomic Mutation
- Two cases of 17α-hydroxylase/17,20-lyase deficiency caused by the CYP17A1 mutation
- A familial case with brachydactyly type C with a GDF5 mutation
