Application of Three-Dimensional Volumetric Ultrasonography in Patients with Bladder Cancer and Its Mimickers: A Pictorial Essay
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Seoul Hospital, Seoul, Korea. hongses@schmc.ac.kr
- KMID: 2377038
- DOI: http://doi.org/10.3348/jksr.2017.76.5.346
Abstract
- Various diseases of the urinary bladder can be demonstrated as being polypoid, a nodular bladder mass or as focal bladder wall thickening. This includes malignant or benign neoplasms, urinary stones, or other inflammatory bladder conditions. In daily practice many of these bladder diseases are easily confused with bladder cancer. On the other hand, ultrasonography (US) is safe and can be easily applied as a screening modality or an initial evaluating tool for urinary bladder disease. Furthermore, additional three-dimensional (3D) volumetric techniques can support more delicate delineation of these lesions. This study presents a 3D volumetric US for bladder lesions, and demonstrates various pathological conditions of the urinary bladder ranging from bladder cancer to other benign lesions.
MeSH Terms
Figure
-
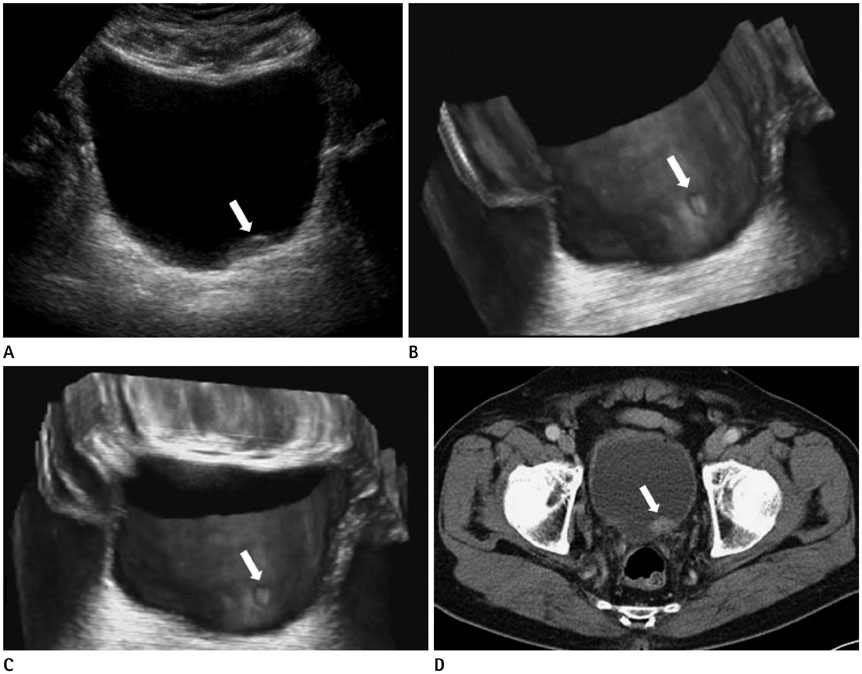
Fig. 1 Superficial polypoid bladder tumor. A. 2D US reveals a tiny echogenic elevated bladder lesion (arrow) with indistinct margin. B, C. 3D US demonstrates the bladder nodule (arrow) with a clearer demarcation. D. Enhanced CT scan shows a well-enhanced polypoid bladder nodule (arrow) at the bladder base. CT = computed tomography, US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional

Fig. 2 Multiple superficial polypoid bladder tumors. A. 2D US of a collapsed bladder showing unclear polypoid bladder nodules. B. 2D US after bladder filling, three polypoid bladder nodules (arrows) are noted. C, D. 3D US clarified three bladder masses (arrows) at a similar site. An additional bladder nodule (arrowheads) is newly identified, which was not detected on the 2D US. The new bladder nodule was confirmed by conventional cystoscopy. US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional
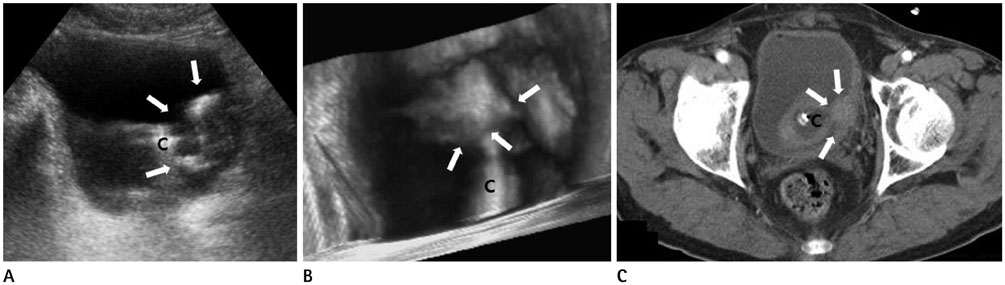
Fig. 3 Bladder mass with indwelling urinary catheter. A. 2D US reveals an echogenic bladder mass (arrows) in a matching site, but contour of the bladder tumor is ambiguous, owing to the urinary catheter (C). B. 3D US provides clearer information about the margin and size of the bladder tumor (arrows) and clarifies the relationship between the tumor and the catheter (C). C. Enhanced CT scan shows a well enhancing bladder mass (arrows) along the left lateral wall of the urinary bladder, which is adjacent to the urinary catheter (C). CT = computed tomography, US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional
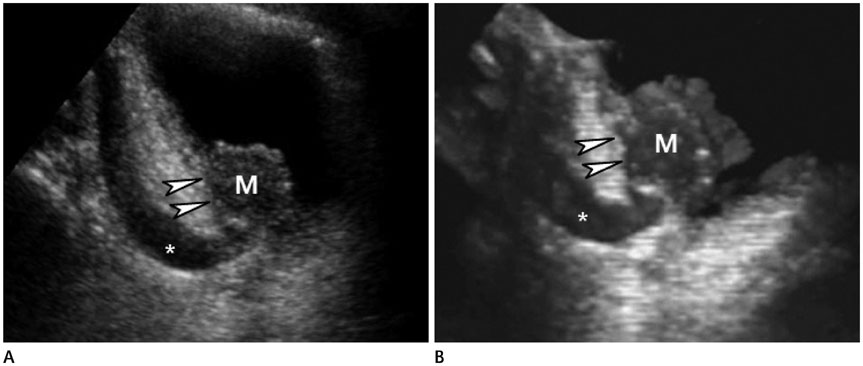
Fig. 4 Infiltrative bladder cancer in UVJ with hydroureter. A. At the sagittal plane of a 2D US, a round hypoechoic bladder mass (M) is identified at the left ureterovesical junction with an obstructive left hydroureterer (*). The outer contour of the urinary bladder (arrowheads) looks smooth, which suggests it has not yet progressed to a stage T2 bladder tumor. B. 3D US revealed that the outer wall (arrowheads) of the urinary bladder was irregular just beside the bladder mass (arrowheads) with an obstructive left hydroureter (*). These findings are suggestive of perivesical invasion (T3). The lesion was confirmed by surgery and pathologically reported as a perivesical invasion. US = ultrasonography, UVJ = ureterovesical junction, 2D = two-dimensional, 3D = three-dimensional
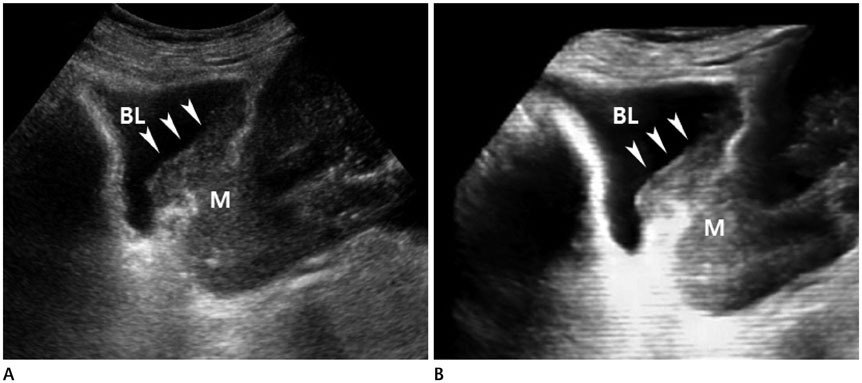
Fig. 5 Direct invasion of the urinary bladder by advanced cervical cancer. A. 2D US shows a large ill-defined uterine cervical mass (M) extending to the bladder (BL) wall (arrowheads). B. 3D US demonstrates the margin of bladder mass more clearly than a conventional 2D US technique (arrowheads). US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional
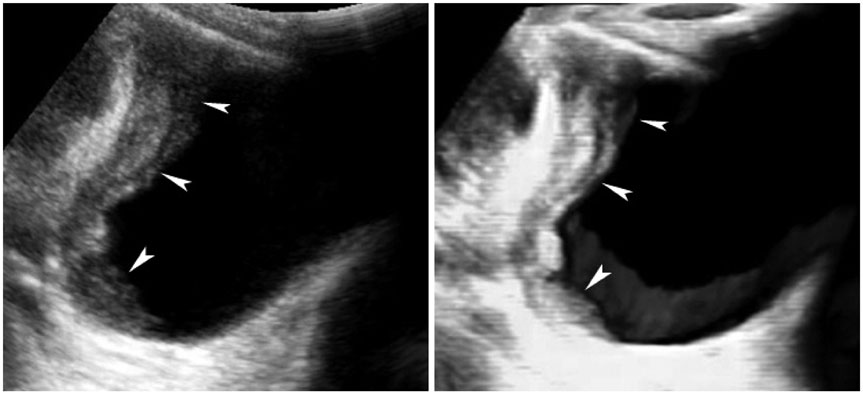
Fig. 6 Metastatic bladder adenocarcinoma from advanced gastric cancer. 2D US and 3D US show diffuse infiltrative masses (arrowheads), confirmed to be have metastasized from gastric cancer to the lateral wall of the urinary bladder. US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional

Fig. 7 Focal cystitis. A. 2D US reveals multiple elevated nodular bladder lesions (arrows) with an indistinct margin. B. 3D US more clearly demonstrates bladder mucosal nodularity (arrows) than 2D US. US = ultrasonography, 2D = two-dimensional, 3D = three-dimensional
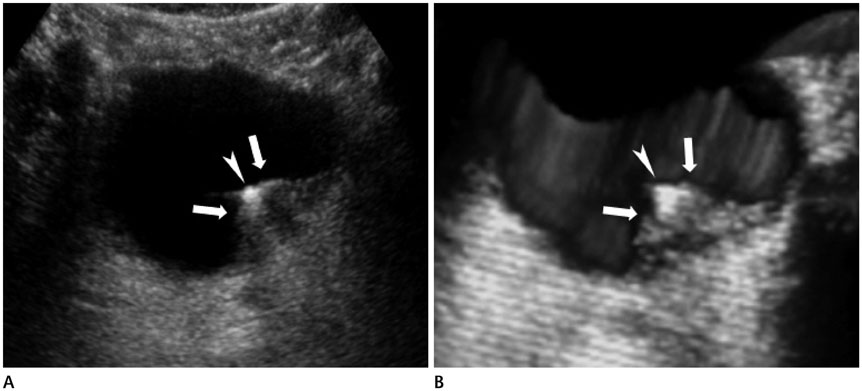
Fig. 8 A left UVJ stone. A. 2D US shows a small echogenic urinary stone (arrowhead) at the left ureterovesical junction with swelling of the surrounding soft tissue (arrows). B. 3D US demarcates the urinary stone (arrowhead) and swelling of left UVJ (arrows) more clearly. US = ultrasonography, UVJ = ureterovesical junction, 2D = two-dimensional, 3D = three-dimensional
Reference
-
1. Ng CS. Radiologic diagnosis and staging of renal and bladder cancer. Semin Roentgenol. 2006; 41:121–138.2. Wagner B, Nesslauer T, Bartsch G Jr, Hautmann RE, Gottfried HW. Staging bladder carcinoma by three-dimensional ultrasound rendering. Ultrasound Med Biol. 2005; 31:301–305.3. Silva-Ramos M, Louro N, Versos R, Cavadas V, Marcelo F. Does 3D ultrasound enhance the diagnosis of bladder tumours in patients with haematuria? ISRN Urol. 2012; 2012:158437.4. Kocakoc E, Kiris A, Orhan I, Poyraz AK, Artas H, Firdolas F. Detection of bladder tumors with 3-dimensional sonography and virtual sonographic cystoscopy. J Ultrasound Med. 2008; 27:45–53.5. Moon MH, Kim SH, Lee YH, Cho JY, Jung SI, Park SH, et al. Diagnostic potential of three-dimensional ultrasound-based virtual cystoscopy: an experimental study using pig bladders. Invest Radiol. 2006; 41:883–889.6. Downey DB, Fenster A, Williams JC. Clinical utility of three-dimensional US. Radiographics. 2000; 20:559–571.7. Wong-You-Cheong JJ, Woodward PJ, Manning MA, Sesterhenn IA. From the Archives of the AFIP: neoplasms of the urinary bladder: radiologic-pathologic correlation. Radiographics. 2006; 26:553–580.8. Pashos CL, Botteman MF, Laskin BL, Redaelli A. Bladder cancer: epidemiology, diagnosis, and management. Cancer Pract. 2002; 10:311–322.9. Vikram R, Sandler CM, Ng CS. Imaging and staging of transitional cell carcinoma: part 1, lower urinary tract. AJR Am J Roentgenol. 2009; 192:1481–1487.10. Cochlin DL, Dubbins PA, Goldberg BB, Halpern EJ. Urogenital Ultrasound: a text atlas. 2nd ed. London: Taylor and Francis;2006. p. 147–150.11. Park HJ, Hong SS, Kim JH, Kwon SB, Kwon KH, Choi DL, et al. Tumor detection and serosal invasion of bladder cancer: role of three-dimensional volumetric reconstructed US. Abdom Imaging. 2010; 35:265–270.12. Lee R, Droller MJ. The natural history of bladder cancer. Implications for therapy. Urol Clin North Am. 2000; 27:1–13. vii13. O'Brien T, Cranston D, Fuggle S, Bicknell R, Harris AL. Different angiogenic pathways characterize superficial and invasive bladder cancer. Cancer Res. 1995; 55:510–513.14. Huang WC, Yang JM, Yang YC, Yang SH. Ultrasonographic characteristics and cystoscopic correlates of bladder wall invasion by endophytic cervical cancer. Ultrasound Obstet Gynecol. 2006; 27:680–686.15. Nyam DC, Seow-Choen F, Ho MS, Goh HS. Bladder involvement in patients with colorectal carcinoma. Singapore Med J. 1995; 36:525–526.16. Kim HC, Kim SH, Hwang SI, Lee HJ, Han JK. Isolated bladder metastases from stomach cancer: CT demonstration. Abdom Imaging. 2001; 26:333–335.17. Baxter GM, Sidhu PS. Ultrasound of the urogenital system. New York: Thieme;2006. p. 137–138.18. Resnick MI, Older RA. Diagnosis of genitourinary disease. New York: George Thieme Verlag;1997. p. 588.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Navigated intraoperative ultrasonography for brain tumors: a pictorial essay on the technique, its utility, and its benefits in neuro-oncology
- Sonographic Features of Palpable Breast and Axillary Lesions in Adult Male Patients: A Pictorial Essay
- Unusual, but important, peri- and extra-articular manifestations of rheumatoid arthritis: a pictorial essay
- Breast lesions during pregnancy and lactation: a pictorial essay
- Imaging Features of Inflammatory Breast Disorders: A Pictorial Essay
