Korean J Endocr Surg.
2013 Jun;13(2):87-91. 10.0000/kjes.2013.13.2.87.
A Comparative Analysis of Endoscopic Versus Conventional Open Thyroidectomy in the Treatment of Papillary Thyroid Cancer According to Preoperative Risk Stratification
- Affiliations
-
- 1Department of Surgery, Konkuk University School of Medicine, Seoul, Korea. kspark@kuh.ac.kr
- KMID: 2375420
- DOI: http://doi.org/10.0000/kjes.2013.13.2.87
Abstract
- PURPOSE
It is well known that papillary thyroid cancer (PTC) has a good prognosis and high incidence in young women. The objective of the study was to review our criteria to select surgical modality and surgical results and to confirm the feasibility of endoscopic thyroidectomy according to the preoperative risk stratification in the treatment of papillary thyroid cancer.
METHODS
Between May 2009 and April 2012, 197 patients underwent either a conventional open or an endoscopic thyroidectomy with the preoperative consideration of risk group using clinical parameters of AMES system (patient age, size of tumor, extrathyroid extension, and presence of distant metastasis). A retrospective analysis of the pathologic data according to AMES system after surgery was also conducted. The endoscopic thyroidectomy was performed using the BABA (bilateral axillo-breast approach) method.
RESULTS
Based on the method of operation, the low-risk group patients (n=197) were divided into two groups: endoscopic group (n=78) and open group (n=119). Procedure time, postoperative complication rates, and length of hospital stay were tracked, albeit these were not significantly different between the two groups. From the pathologic findings, it was reported that there were no significant differences in tumor size, extrathyroid extension, and metastasis and also in the Off T4 - thyroglobulin level between the two groups.
CONCLUSION
Endoscopic thyroidectomy is a feasible method for the treatment of selected cases of thyroid cancer such as low-risk group according to the appropriate preoperative risk stratification.
MeSH Terms
Figure
-
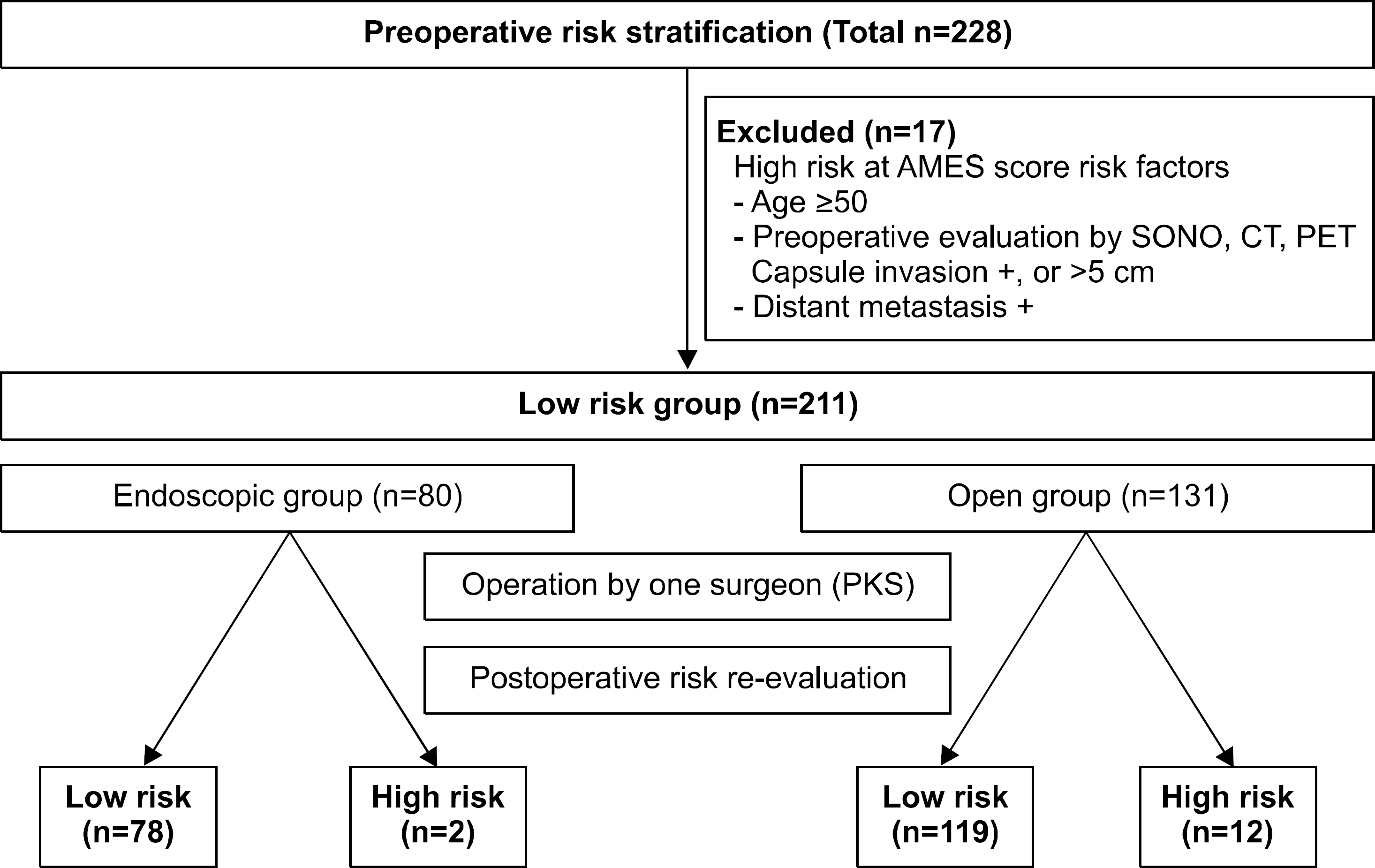
Fig. 1. Flowchart of this study design.
Reference
-
References
1. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009; 19:1167–214.
Article2. Ikeda Y, Takami H, Sasaki Y, Kan S, Niimi M. Endoscopic resection of thyroid tumors by the axillary approach. J Cardiovasc Surg (Torino). 2000; 41:791–2.3. Hüscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997; 11:877.
Article4. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillobreast approach. World J Surg. 2007; 31:601–6.
Article5. Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg. 2007; 31:2302–6.
Article6. Choi JY, Lee KE, Chung KW, Kim SW, Choe JH, Koo do H, et al. Endoscopic thyroidectomy via bilateral axillobreast approach (BABA): review of 512 cases in a single institute. Surg Endosc. 2012; 26:948–55.
Article7. Lee KE, Rao J, Youn YK. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech. 2009; 19:e71–5.8. Jeong JJ, Kang SW, Yun JS, Sung TY, Lee SC, Lee YS, et al. Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol. 2009; 100:477–80.
Article9. Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Gasless endoscopic thyroidectomy using transaxillary approach; surgical outcome of 581 patients. Endocr J. 2009; 56:361–9.
Article10. Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009; 23:2399–406.
Article11. Lee KE, Koo do H, Kim SJ, Lee J, Park KS, Oh SK, et al. Outcomes of 109 patients with papillary thyroid carcinoma who underwent robotic total thyroidectomy with central node dissection via the bilateral axillobreast approach. Surgery. 2010; 148:1207–13.
Article12. Kim SJ, Lee KE, Choe JH, Lee J, Koo do H, Oh SK, et al. Endoscopic completion thyroidectomy by the bilateral axillobreast approach. Surg Laparosc Endosc Percutan Tech. 2010; 20:312–6.
Article13. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007; 57:43–66.
Article14. Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Park EC, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2008. Cancer Res Treat. 2011; 43:1–11.
Article15. Mazzaferri EL. Long-term outcome of patients with differentiated thyroid carcinoma: effect of therapy. Endocr Pract. 2000; 6:469–76.
Article16. Nixon IJ, Ganly I, Patel SG, Palmer FL, Whitcher MM, Tuttle RM, et al. Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery. 2012; 151:571–9.
Article17. Bilimoria KY, Bentrem DJ, Ko CY, Stewart AK, Winchester DP, Talamonti MS, et al. Extent of surgery affects survival for papillary thyroid cancer. Ann Surg. 2007; 246:375–81.
Article18. Cady B, Rossi R. An expanded view of risk-group definition in differentiated thyroid carcinoma. Surgery. 1988; 104:947–53.19. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993; 114:1050–7.20. Voutilainen PE, Siironen P, Franssila KO, Sivula A, Haapiainen RK, Haglund CH. AMES, MACIS and TNM prognostic classifications in papillary thyroid carcinoma. Anticancer Res. 2003; 23:4283–8.21. Xing M, Westra WH, Tufano RP, Cohen Y, Rosenbaum E, Rhoden KJ, et al. BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. J Clin Endocrinol Metab. 2005; 90:6373–9.
Article22. Durante C, Attard M, Torlontano M, Ronga G, Monzani F, Costante G, et al. Papillary Thyroid Cancer Study Group. Identification and optimal postsurgical follow-up of patients with very low-risk papillary thyroid microcarcinomas. J Clin Endocrinol Metab. 2010; 95:4882–8.
Article23. Shaha AR, Shah JP, Loree TR. Low-risk differentiated thyroid cancer: the need for selective treatment. Ann Surg Oncol. 1997; 4:328–33.
Article24. Mazzaferri EL. Management of low-risk differentiated thyroid cancer. Endocr Pract. 2007; 13:498–512.
Article25. Lo CY, Chan WF, Lam KY, Wan KY. Optimizing the treatment of AMES high-risk papillary thyroid carcinoma. World J Surg. 2004; 28:1103–9.
Article26. Miccoli P, Pinchera A, Materazzi G, Biagini A, Berti P, Faviana P, et al. Surgical treatment of low- and intermediate-risk papillary thyroid cancer with minimally invasive video-assisted thyroidectomy. J Clin Endocrinol Metab. 2009; 94:1618–22.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A comparative analysis of endoscopic thyroidectomy versus conventional thyroidectomy in clinically lymph node negative thyroid cancer
- Subcutaneous Soft Tissue Implantation of Papillary Thyroid Carcinoma after Endoscopic Thyroidectomy
- Transaxillary Endoscopic Thyroidectomy versus Conventional Open Thyroidectomy for Papillary Thyroid Cancer: 5-year Surgical Outcomes
- Thyroid Lobectomy as an Initial Treatment Option on 1-4 cm Papillary Cancer
- Endoscopic Thyroidectomy in Thyroid Cancer
