Granulocytic Sarcoma in Breast after Bone Marrow Transplantation
- Affiliations
-
- 1Special Study Module for Breast, Ajou University School of Medicine, Suwon, Korea.
- 2Department of Surgery, Ajou University School of Medicine, Suwon, Korea. ideakims@gmail.com
- 3Department of Hematology-Oncology, Ajou University School of Medicine, Suwon, Korea.
- 4Department of Radiology, Ajou University School of Medicine, Suwon, Korea.
- 5Department of Pathology, Ajou University School of Medicine, Suwon, Korea.
- 6Department of Biomedical Informatics, Ajou University School of Medicine, Suwon, Korea.
Abstract
- Granulocytic sarcoma is a localized extramedullary solid tumor composed of immature myeloid cell and is usually associated with acute myeloid leukemia or myelodysplastic syndrome. Although it can involve any site, commonly in lymph nodes, skin, bone and soft tissue, the involvement of breast is unusual. Especially, the involvement of the breast as a pattern of relapse after bone marrow transplantation is extremely rare. We have experienced 2 cases of granulocytic sarcoma after bone marrow transplantation. One case was a 39-year-old woman with right breast mass diagnosed with granulocytic sarcoma. She had received an unrelated bone marrow transplantation due to biphenotype acute leukemia 3 years before our presentation. Another case was a 48-year-old woman with acute myeloid leukemia, who was diagnosed with granulocytic sarcoma on both breasts 8 months after allogenic bone marrow transplantation. We also discuss the clinicopathologic features of granulocytic sarcoma in breast after bone marrow transplantation.
Keyword
MeSH Terms
Figure
-

Figure 1 Case 1. Ultrasonographic images of right breast (A) and axilla (B). Heterogenous hypoechoic masses with multifocal cystic portion in entire right breast with right axillary lymphadenopathy were identified.
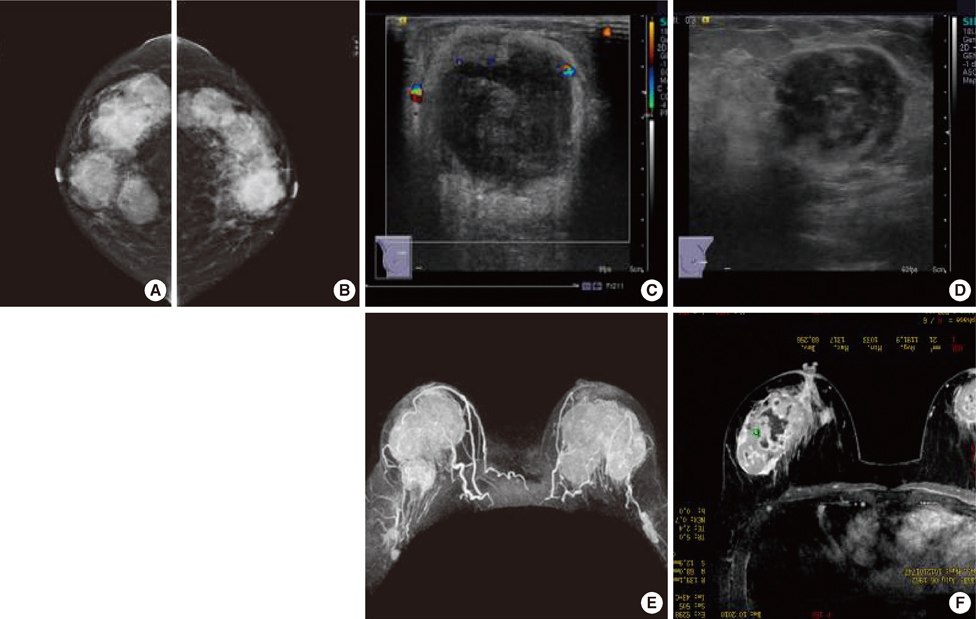
Figure 2 Case 2. Radiologic findings of the breast. (A, B) Mammograms show multiple various sized circumscribed and ill defined iso to hypodense masses at both breast (A, right craniocaudal view; B, left craniocaudal view). (C, D) Sonographic images show multiple heterogeneous hypoechoic masses with echogenic boundary at both breast (C, right; D, left). (E, F) Magnetic resonance imaging findings show multiple variable sized enhancing masses in both breasts (E) and most of them show internal necrotic portion (F).

Figure 3 (A) Microscopic finding of case 2 shows diffuse infiltration of myeloblast (H&E stain, ×200). (B) Neoplastic cells were immunoreactive (purple stained area) for myeloperoxidase (immunohistochemistry stain, ×400).
Reference
-
1. Neiman RS, Barcos M, Berard C, Bonner H, Mann R, Rydell RE, et al. Granulocytic sarcoma: a clinicopathologic study of 61 biopsied cases. Cancer. 1981. 48:1426–1437.
Article2. Wiernik PH, Serpick AA. Granulocytic sarcoma (chloroma). Blood. 1970. 35:361–369.
Article3. Baer MR. Management of unusual presentations of acute leukemia. Hematol Oncol Clin North Am. 1993. 7:275–292.
Article4. Breccia M, Mandelli F, Petti MC, D'Andrea M, Pescarmona E, Pileri SA, et al. Clinico-pathological characteristics of myeloid sarcoma at diagnosis and during follow-up: report of 12 cases from a single institution. Leuk Res. 2004. 28:1165–1169.
Article5. Ngu IW, Sinclair EC, Greenaway S, Greenberg ML. Unusual presentation of granulocytic sarcoma in the breast: a case report and review of the literature. Diagn Cytopathol. 2001. 24:53–57.
Article6. Pileri SA, Ascani S, Cox MC, Campidelli C, Bacci F, Piccioli M, et al. Myeloid sarcoma: clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia. 2007. 21:340–350.
Article7. Viadana E, Bross ID, Pickren JW. An autopsy study of the metastatic patterns of human leukemias. Oncology. 1978. 35:87–96.
Article8. Liu PI, Ishimaru T, McGregor DH, Okada H, Steer A. Autopsy study of granulocytic sarcoma (chloroma) in patients with myelogenous leukemia, Hiroshima-Nagasaki 1949-1969. Cancer. 1973. 31:948–955.
Article9. Joo M, Lee HK, Kang YK, Kim JH. Granulocytic sarcoma of the breast preceding acute myelogenous leukemia: a case report. J Korean Med Sci. 2000. 15:457–459.
Article10. Park SK, Suh SH, Nam HK, Kang AY, Kim DC, Han JY, et al. A case of granulocytic sarcoma relapsed in both breasts after complete remission of acute myelogeous leukemia. Korean J Lab Med. 2005. 25:223–226.11. Békássy AN, Hermans J, Gorin NC, Gratwohl A. Granulocytic sarcoma after allogeneic bone marrow transplantation: a retrospective European multicenter survey. Acute and Chronic Leukemia Working Parties of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 1996. 17:801–808.12. Basara I, Orguc S. Giant breast involvement in acute lymphoblastic leukemia: MRI findings. J Breast Cancer. 2012. 15:258–260.
Article13. Markoc F, Bozdogan N, Yükrük FA, Gumuc EB, Akdur NC. Granulocytic sarcomas: difficulties in diagnosis. Tumori. 2010. 96:149–153.
Article14. Chua ET. A case of granulocytic sarcoma of the breast and review of the literature. Singapore Med J. 1989. 30:311–312.15. Monteleone PM, Steele DA, King AK, Konefal S, Kelleher JF. Bilateral breast relapse in acute myelogenous leukemia. J Pediatr Hematol Oncol. 2001. 23:126–129.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cases of extramedullary relapse after alloBMT in AML1/ETO positive AML
- Metastatic Granulocytic Sarcoma in the Breast: A Case Report
- A Case of Granulocytic Sarcoma Involving the Forniceal Conjunctiva
- A Case of Orbital Granulocytic Sarcoma
- A case of donor-derived granulocytic sarcoma after allogeneic hematopoietic stem cell transplantation
