Extremely Well-Differentiated Papillary Thyroid Carcinoma Resembling Adenomatous Hyperplasia Can Metastasize to the Skull: A Case Report
- Affiliations
-
- 1Department of Pathology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. soonwonh@yuhs.ac
- 2Department of Pathology, CHA Gangnam Hospital, CHA University Medical School, Seoul, Korea.
- 3Department of Pathology, Yonsei MokGu Clinic, Seosan, Korea.
- 4Thyroid Cancer Center, Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2374215
- DOI: http://doi.org/10.3349/ymj.2017.58.1.255
Abstract
- We describe herein histologic, immunohistochemical, and molecular findings and clinical manifestations of a rare case of an extremely well differentiated papillary thyroid carcinoma (EWD-PTC). Similarly, it is also difficult to diagnose follicular variant papillary thyroid carcinoma (FVPTC), whose diagnosis is still met with controversy. A recently reported entity of well-differentiated tumor of uncertain malignant potential (WDT-UMP) is added to the diagnostic spectrum harboring EWD-PTC and FVPTC. We report this case, because EWD-PTC is different from FVPTC in its papillary architecture, and also from WDT-UMP in its recurrence and metastatic pattern. These morphologically deceptive entities harbored diagnostic difficulties in the past because the diagnosis depended solely on histology. However, they are now diagnosed with more certainty by virtue of immunohistochemical and molecular studies. We experienced a case of EWD-PTC, which had been diagnosed as adenomatous hyperplasia 20 years ago and manifested recurrence with lymph node (LN) metastasis 7 years later. After another 7 years of follow-up, a new thyroid lesion had developed, diagnosed as FVPTC, with LN metastasis of EWD-PTC. One year later, the patient developed metastatic FVPTC in the skull. Immunohistochemically, the EWD-PTC was focally positive for CK19, negative for galectin-3, and focally negative for CD56. Molecular studies revealed BRAF-positivity and K-RAS negativity. The FVPTC in the left thyroid showed both BRAF and K-RAS negativity. In conclusion, EWD-PTC and FVPTC share similar histologic features, but they are different tumors with different molecular biologic and clinical manifestations. A large cohort of EWD-PTC should be included in further study.
Keyword
MeSH Terms
Figure
-
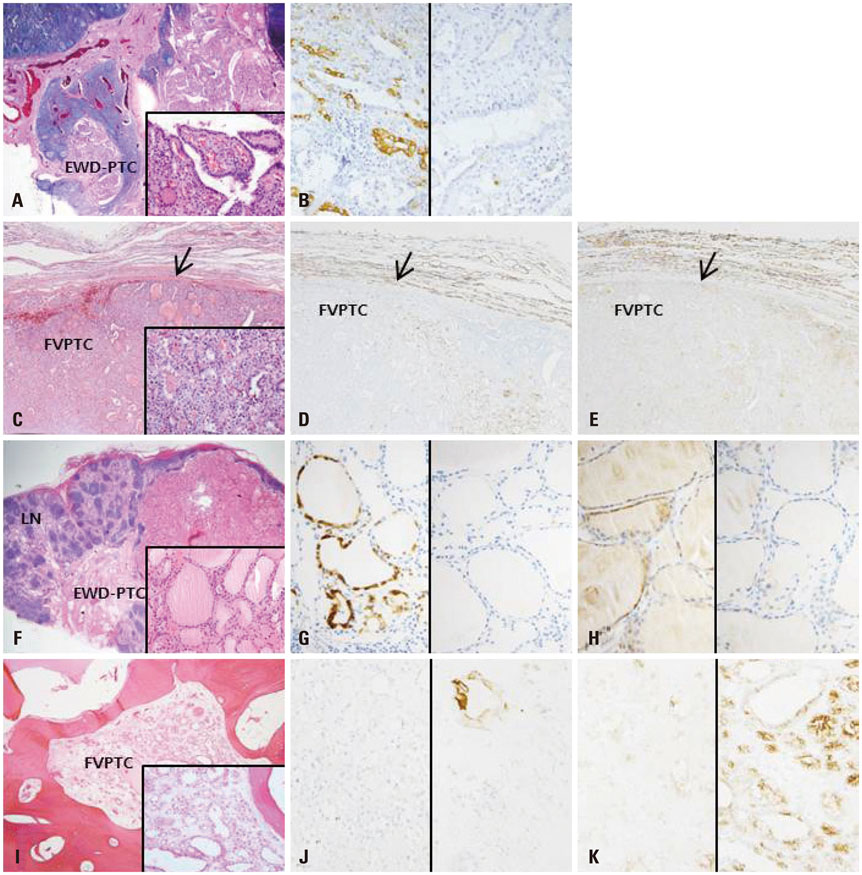
Fig. 1 Neck lymph node (LN) shows metastatic extremely well differentiated papillary thyroid carcinoma (EWD-PTC) (A, H-E stain, ×12.5 and inset ×400) with focal positivity of CK19 (B, ×400) in the first metastatic lesion. The left thyroid shows follicular variant papillary thyroid carcinoma (FVPTC) without capsular (arrow) invasion (C, H-E stain, ×40 and inset ×400) with focal positivity of CK19 (D, ×40) and loss of CD56 (E, ×40) in second episode. The LN also shows metastatic EWD-PTC (F, H-E stain, ×12.5 and inset ×400) with focal positivity of CK19 (G, ×400) and CD56 (H, ×400) in the second metastatic lesion. The skull lesion shows metastatic FVPTC (I, H-E stain, ×100 and inset ×400) with focal positivity of CK19 (J, ×400) and CD56 (K, ×400).
Reference
-
1. Kesmodel SB, Terhune KP, Canter RJ, Mandel SJ, LiVolsi VA, Baloch ZW, et al. The diagnostic dilemma of follicular variant of papillary thyroid carcinoma. Surgery. 2003; 134:1005–1012.
Article2. Lloyd RV, Erickson LA, Casey MB, Lam KY, Lohse CM, Asa SL, et al. Observer variation in the diagnosis of follicular variant of papillary thyroid carcinoma. Am J Surg Pathol. 2004; 28:1336–1340.
Article3. Yassin Fel-Z. Diagnostic criteria of well differentiated thyroid tumor of uncertain malignant potential; a histomorphological and immunohistochemical appraisal. J Egypt Natl Canc Inst. 2015; 27:59–67.
Article4. Nechifor-Boila A, Borda A, Sassolas G, Hafdi-Nejjari Z, Cătană R, Borson-Chazot F, et al. Thyroid tumors of uncertain malignant potential: morphologic and imunohistochemical analysis of 29 cases. Pathol Res Pract. 2015; 211:320–325.
Article5. Noh BJ, Sung JY, Kim YW, Park YK. Recurrent thyroid papillary carcinoma in children under ten years old: report of two cases and literature review. Korean J Pathol. 2014; 48:297–301.
Article6. Choi SE, Hong SW, Yoon SO. Proposal of an appropriate decalcification method of bone marrow biopsy specimens in the era of expanding genetic molecular study. J Pathol Transl Med. 2015; 49:236–242.
Article7. Lin HS, Komisar A, Opher E, Blaugrund SM. Follicular variant of papillary carcinoma: the diagnostic limitations of preoperative fine-needle aspiration and intraoperative frozen section evaluation. Laryngoscope. 2000; 110:1431–1436.
Article8. Liu FH, Liou MJ, Hsueh C, Chao TC, Lin JD. Thyroid follicular neoplasm: analysis by fine needle aspiration cytology, frozen section, and histopathology. Diagn Cytopathol. 2010; 38:801–805.
Article9. Ma H, Yan J, Zhang C, Qin S, Qin L, Liu L, et al. Expression of papillary thyroid carcinoma-associated molecular markers and their significance in follicular epithelial dysplasia with papillary thyroid carcinoma-like nuclear alterations in Hashimoto’s thyroiditis. Int J Clin Exp Pathol. 2014; 7:7999–8007.10. Hofman V, Lassalle S, Bonnetaud C, Butori C, Loubatier C, Ilie M, et al. Thyroid tumours of uncertain malignant potential: frequency and diagnostic reproducibility. Virchows Arch. 2009; 455:21–33.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adenomatous Hyperplasia Arising from Dual Ectopic Thyroid
- Papillary Carcinoma of Thyroid in Association with Familial Adenomatous Polyposis
- Concurrent Medullay and Papillary Carcinoma of the Thyroid
- A Novel Adenomatous Polyposis Coli Gene Mutation of Cribriform-Morular Variant Papillary Thyroid Carcinoma: A Case Report
- Cribriform-Morular Variant of Papillary Thyroid Carcinoma Associated with Familial Adenomatous Polyposis
