Yonsei Med J.
2016 Jul;57(4):824-830. 10.3349/ymj.2016.57.4.824.
Re-Irradiation for Recurrent Gliomas: Treatment Outcomes and Prognostic Factors
- Affiliations
-
- 1Department of Radiation Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Korea. cosuh317@yuhs.ac
- 2Department of Neurosurgery, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Korea. changjh@yuhs.ac
- KMID: 2374111
- DOI: http://doi.org/10.3349/ymj.2016.57.4.824
Abstract
- PURPOSE
The aim of this study was to evaluate the efficacy of re-irradiation in patients with recurrent gliomas and to identify subgroups for whom re-irradiation for recurrent gliomas is most beneficial.
MATERIALS AND METHODS
We retrospectively reviewed 36 patients with recurrent or progressive gliomas who received re-irradiation between January 1996 and December 2011. Re-irradiation was offered to recurrent glioma patients with good performance or at least 6 months had passed after initial radiotherapy (RT), with few exceptions.
RESULTS
Median doses of re-irradiation and initial RT were 45.0 Gy and 59.4 Gy, respectively. The median time interval between initial RT and re-irradiation was 30.5 months. Median overall survival (OS) and the 12-month OS rate were 11 months and 41.7%, respectively. In univariate analysis, Karnofsky performance status (KPS) ≥70 (p<0.001), re-irradiation dose ≥45 Gy (p=0.040), and longer time interval between initial RT and re-irradiation (p=0.040) were associated with improved OS. In multivariate analysis, KPS (p=0.030) and length of time interval between initial RT and re-irradiation (p=0.048) were important predictors of OS. A radiographically suspected mixture of radiation necrosis and progression after re-irradiation was seen in 5 patients.
CONCLUSION
Re-irradiation in conjunction with surgery could be a salvage treatment for selected recurrent glioma patients with good performance status and recurrence over a long time.
Keyword
MeSH Terms
-
Adult
Brain Neoplasms/mortality/*radiotherapy/surgery
Female
Glioma/mortality/*radiotherapy/surgery
Humans
Karnofsky Performance Status
Male
Middle Aged
Multivariate Analysis
Neoplasm Recurrence, Local/mortality/*radiotherapy/surgery
*Re-Irradiation
Retrospective Studies
Salvage Therapy
Treatment Outcome
Young Adult
Figure
-
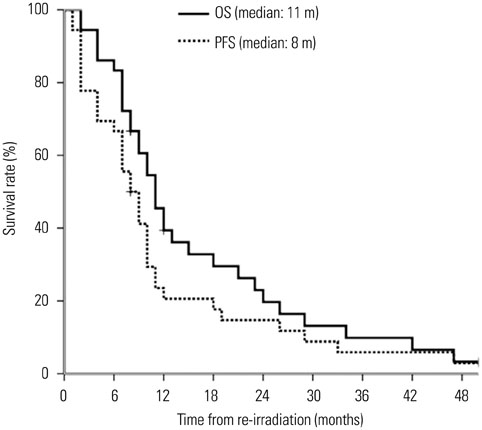
Fig. 1 Overall survival (OS) and progression-free survival (PFS) for recurrent glioma patients treated with re-irradiation.

Fig. 2 Overall survival for recurrent glioma patients with different Karnofsky performance status (KPS) categories who received re-irradiation.
Cited by 1 articles
-
Hypofractionated Re-irradiation after Maximal Surgical Resection for Recurrent Glioblastoma: Therapeutic Adequacy and Its Prognosticators of Survival
Jeongshim Lee, Sung Soo Ahn, Jong Hee Chang, Chang-Ok Suh
Yonsei Med J. 2018;59(2):194-201. doi: 10.3349/ymj.2018.59.2.194.
Reference
-
1. Wallner KE, Galicich JH, Krol G, Arbit E, Malkin MG. Patterns of failure following treatment for glioblastoma multiforme and anaplastic astrocytoma. Int J Radiat Oncol Biol Phys. 1989; 16:1405–1409.
Article2. Brandes AA, Tosoni A, Franceschi E, Sotti G, Frezza G, Amistà P, et al. Recurrence pattern after temozolomide concomitant with and adjuvant to radiotherapy in newly diagnosed patients with glioblastoma: correlation With MGMT promoter methylation status. J Clin Oncol. 2009; 27:1275–1279.
Article3. Milano MT, Okunieff P, Donatello RS, Mohile NA, Sul J, Walter KA, et al. Patterns and timing of recurrence after temozolomide-based chemoradiation for glioblastoma. Int J Radiat Oncol Biol Phys. 2010; 78:1147–1155.
Article4. Dobelbower MC, Burnett Iii OL, Nordal RA, Nabors LB, Markert JM, Hyatt MD, et al. Patterns of failure for glioblastoma multiforme following concurrent radiation and temozolomide. J Med Imaging Radiat Oncol. 2011; 55:77–81.
Article5. Sherriff J, Tamangani J, Senthil L, Cruickshank G, Spooner D, Jones B, et al. Patterns of relapse in glioblastoma multiforme following concomitant chemoradiotherapy with temozolomide. Br J Radiol. 2013; 86:20120414.
Article6. Dirks P, Bernstein M, Muller PJ, Tucker WS. The value of reoperation for recurrent glioblastoma. Can J Surg. 1993; 36:271–275.7. Franceschi E, Omuro AM, Lassman AB, Demopoulos A, Nolan C, Abrey LE. Salvage temozolomide for prior temozolomide responders. Cancer. 2005; 104:2473–2476.
Article8. Vredenburgh JJ, Desjardins A, Herndon JE 2nd, Marcello J, Reardon DA, Quinn JA, et al. Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J Clin Oncol. 2007; 25:4722–4729.
Article9. Chinot OL, Honore S, Dufour H, Barrie M, Figarella-Branger D, Muracciole X, et al. Safety and efficacy of temozolomide in patients with recurrent anaplastic oligodendrogliomas after standard radiotherapy and chemotherapy. J Clin Oncol. 2001; 19:2449–2455.
Article10. Wong ET, Hess KR, Gleason MJ, Jaeckle KA, Kyritsis AP, Prados MD, et al. Outcomes and prognostic factors in recurrent glioma patients enrolled onto phase II clinical trials. J Clin Oncol. 1999; 17:2572–2578.
Article11. Yung WK, Prados MD, Yaya-Tur R, Rosenfeld SS, Brada M, Friedman HS, et al. Multicenter phase II trial of temozolomide in patients with anaplastic astrocytoma or anaplastic oligoastrocytoma at first relapse. Temodal Brain Tumor Group. J Clin Oncol. 1999; 17:2762–2771.12. Shepherd SF, Laing RW, Cosgrove VP, Warrington AP, Hines F, Ashley SE, et al. Hypofractionated stereotactic radiotherapy in the management of recurrent glioma. Int J Radiat Oncol Biol Phys. 1997; 37:393–398.
Article13. Hudes RS, Corn BW, Werner-Wasik M, Andrews D, Rosenstock J, Thoron L, et al. A phase I dose escalation study of hypofractionated stereotactic radiotherapy as salvage therapy for persistent or recurrent malignant glioma. Int J Radiat Oncol Biol Phys. 1999; 43:293–298.
Article14. Arcicasa M, Roncadin M, Bidoli E, Dedkov A, Gigante M, Trovò MG. Reirradiation and lomustine in patients with relapsed highgrade gliomas. Int J Radiat Oncol Biol Phys. 1999; 43:789–793.
Article15. Veninga T, Langendijk HA, Slotman BJ, Rutten EH, van der Kogel AJ, Prick MJ, et al. Reirradiation of primary brain tumours: survival, clinical response and prognostic factors. Radiother Oncol. 2001; 59:127–137.
Article16. Vordermark D, Kölbl O, Ruprecht K, Vince GH, Bratengeier K, Flentje M. Hypofractionated stereotactic re-irradiation: treatment option in recurrent malignant glioma. BMC Cancer. 2005; 5:55.
Article17. Gutin PH, Iwamoto FM, Beal K, Mohile NA, Karimi S, Hou BL, et al. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys. 2009; 75:156–163.
Article18. Fogh SE, Andrews DW, Glass J, Curran W, Glass C, Champ C, et al. Hypofractionated stereotactic radiation therapy: an effective therapy for recurrent high-grade gliomas. J Clin Oncol. 2010; 28:3048–3053.
Article19. Minniti G, Armosini V, Salvati M, Lanzetta G, Caporello P, Mei M, et al. Fractionated stereotactic reirradiation and concurrent temozolomide in patients with recurrent glioblastoma. J Neurooncol. 2011; 103:683–691.
Article20. Niyazi M, Ganswindt U, Schwarz SB, Kreth FW, Tonn JC, Geisler J, et al. Irradiation and bevacizumab in high-grade glioma retreatment settings. Int J Radiat Oncol Biol Phys. 2012; 82:67–76.
Article21. Macdonald DR, Cascino TL, Schold SC Jr, Cairncross JG. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990; 8:1277–1280.
Article22. Hochberg FH, Pruitt A. Assumptions in the radiotherapy of glioblastoma. Neurology. 1980; 30:907–911.
Article23. Combs SE, Thilmann C, Edler L, Debus J, Schulz-Ertner D. Efficacy of fractionated stereotactic reirradiation in recurrent gliomas: longterm results in 172 patients treated in a single institution. J Clin Oncol. 2005; 23:8863–8869.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Appraisal of re-irradiation for the recurrent glioblastoma in the era of MGMT promotor methylation
- Expression of Trans forming Growth Factor-a and Proliferating Cell Nuclear Antigen in Human Gliomas
- Brainstem Gliomas: Classification, Growth Patterns, and Prognosis
- Re-Irradiation and Its Contribution to Good Prognosisin Recurrent Glioblastoma Patients
- Glioma Immunotherapy: Advances and Challenges for Spinal Cord Gliomas
