The Degree of Diabetic Retinopathy in Patients with Type 2 Diabetes Correlates with the Presence and Severity of Coronary Heart Disease
- Affiliations
-
- 1Department of Ophthalmology, 38th Fighter Group Medical Station, Gunsan, Korea.
- 2Department of Ophthalmology, Yonsei Eagle Eye Hospital, Seongnam, Korea.
- 3Department of Ophthalmology, Asan Medical Center, University of Ulsan, College of Medicine, Seoul, Korea. yhyoon@amc.seoul.kr
- 4Department of Radiology, Asan Medical Center, University of Ulsan, College of Medicine, Seoul, Korea.
- 5Department of Radiology, Chonbuk National University Medical School and Hospital, Research Institute of Clinical Medicine, Jeonju, Korea.
- KMID: 2373759
- DOI: http://doi.org/10.3346/jkms.2016.31.8.1292
Abstract
- Both diabetic retinopathy (DR) and coronary heart disease (CHD) are clinically significant in diabetic patients. We investigated the correlation between the severity of DR and the presence and severity of CHD among type 2 diabetic patients. A total of 175 patients who were examined at the DR clinic and underwent dual-source computed tomography (DSCT) angiography within 6 months were included. The degree of DR was graded as no DR, nonproliferative DR (NPDR), and proliferative DR (PDR). The severity of CHD and the numbers of significant stenotic coronary artery on DSCT angiography according to DR grade were assessed. The mean Agatston Calcium Score (ACS) in patients with PDR was significantly higher than other groups (P < 0.001). The overall odds of an ACS increase were about 4.7-fold higher in PDR group than in no DR group (P < 0.001). In PDR group, in comparison with in no DR, the odds of having 1 or 2 arterial involvement were 3-fold higher (P = 0.044), and those of having 3 were 17-fold higher (P = 0.011). The c-index, one of the predictability values in regression analysis model, was not significantly increased when PDR was added to classical CHD risk factors (0.671 to 0.706, P = 0.111). Conclusively, patients with PDR develop a greater likelihood of not only having CHD, but being more severe nature. PDR has no additional effect to classical CHD risk factors for predicting CHD.
MeSH Terms
-
Aged
Angiography
Coronary Artery Disease/complications/*pathology
Coronary Vessels/diagnostic imaging
Diabetes Mellitus, Type 2/*complications
Diabetic Retinopathy/complications/*diagnosis/diagnostic imaging
Female
Glomerular Filtration Rate
Humans
Linear Models
Male
Middle Aged
Odds Ratio
Risk Factors
Severity of Illness Index
Tomography, X-Ray Computed
Figure
-
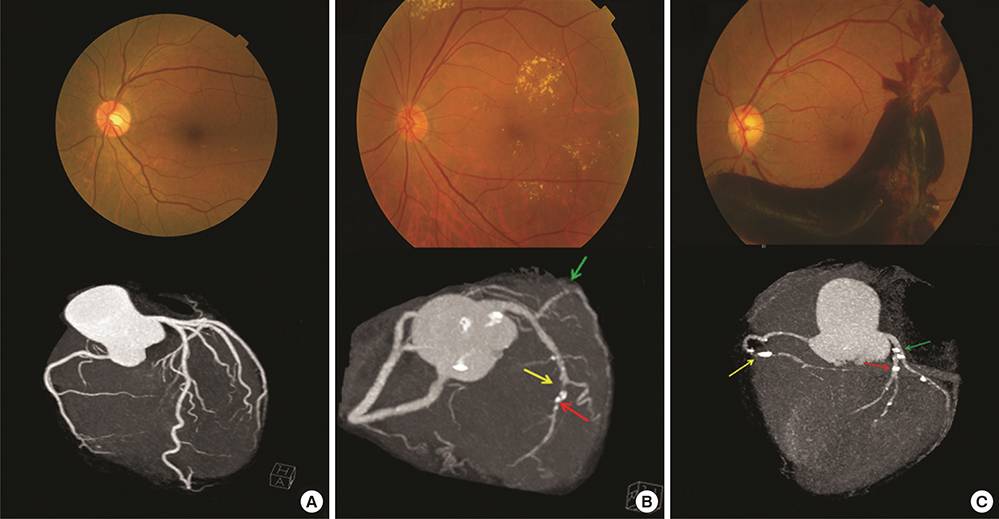
Fig. 1 Fundus photographs and coronary CT images of representative cases in each diabetic retinopathy category. (A) A patient with no DR (top) and no sign of coronary artery stenosis. The total ACS was zero in this case. (B) A patient with NPDR (top) and significant stenosis in the mLAD artery (yellow arrow) and dLCX artery (green arrow). Calcified plaques are evident in the LAD artery (red arrow) and the total ACS of this case was 159.2. (C) A patient with PDR (top) showing significant stenosis in the dRCA (yellow arrow), LAD artery (red arrow) and pLCX artery (green arrow) with heavy calcified plaques. The total ACS in this patient was 374.6. DR, diabetic retinopathy; NPDR, non-proliferative DR; PDR, proliferative DR; ACS, Agatston calcium score; mLAD, mid left anterior descending; dLCX, distal left circumflex; dRCA, distal right coronary artery.
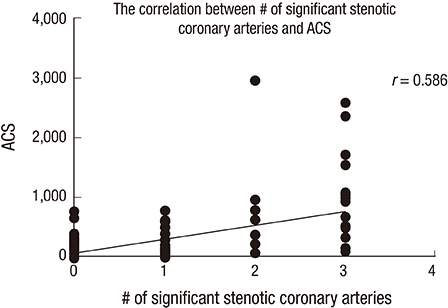
Fig. 2 Correlation between the number of significant stenotic coronary arteries and the ACS. ACS, Agatston calcium score.
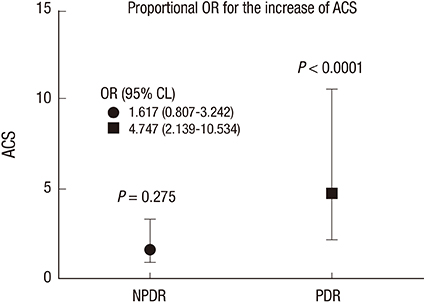
Fig. 3 The proportional odds ratio for increasing ACS between PDR, NPDR and no DR group, respectively. ACS, Agatston calcium score; DR, diabetic retinopathy; NPDR, non-proliferative DR; PDR, proliferative DR.

Fig. 4 Odds ratios for significantly stenotic coronary artery numbers among different DR states. DR: diabetic retinopathy.
Reference
-
1. Consensus development conference on the diagnosis of coronary heart disease in people with diabetes: 10-11 February 1998, Miami, Florida. American Diabetes Association. Diabetes Care. 1998; 21:1551–1559.2. Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998; 339:229–234.3. Cheung N, Wang JJ, Klein R, Couper DJ, Sharrett AR, Wong TY. Diabetic retinopathy and the risk of coronary heart disease: the Atherosclerosis Risk in Communities Study. Diabetes Care. 2007; 30:1742–1746.4. Rosenson RS, Fioretto P, Dodson PM. Does microvascular disease predict macrovascular events in type 2 diabetes? Atherosclerosis. 2011; 218:13–18.5. Targher G, Bertolini L, Zenari L, Lippi G, Pichiri I, Zoppini G, Muggeo M, Arcaro G. Diabetic retinopathy is associated with an increased incidence of cardiovascular events in type 2 diabetic patients. Diabet Med. 2008; 25:45–50.6. Tsujimoto T, Kajio H, Takahashi Y, Kishimoto M, Noto H, Yamamoto-Honda R, Kamimura M, Morooka M, Kubota K, Shimbo T, et al. Asymptomatic coronary heart disease in patients with type 2 diabetes with vascular complications: a cross-sectional study. BMJ Open. 2011; 1:e000139.7. Yoon KC, Mun GH, Kim SD, Kim SH, Kim CY, Park KH, Park YJ, Baek SH, Song SJ, Shin JP, et al. Prevalence of eye diseases in South Korea: data from the Korea National Health and Nutrition Examination Survey 2008-2009. Korean J Ophthalmol. 2011; 25:421–433.8. Kawasaki R, Cheung N, Islam FM, Klein R, Klein BE, Cotch MF, Sharrett AR, O’Leary D, Wong TY; Multi-Ethnic Study of Atherosclerosis. Is diabetic retinopathy related to subclinical cardiovascular disease? Ophthalmology. 2011; 118:860–865.9. Koistinen MJ. Prevalence of asymptomatic myocardial ischaemia in diabetic subjects. BMJ. 1990; 301:92–95.10. Ditchburn CJ, Hall JA, de Belder M, Davies A, Kelly W, Bilous R. Silent myocardial ischaemia in patients with proved coronary artery disease: a comparison of diabetic and non-diabetic patients. Postgrad Med J. 2001; 77:395–398.11. Wong TY, Klein R, Islam FM, Cotch MF, Folsom AR, Klein BE, Sharrett AR, Shea S. Diabetic retinopathy in a multi-ethnic cohort in the United States. Am J Ophthalmol. 2006; 141:446–455.12. Klein R, Sharrett AR, Klein BE, Moss SE, Folsom AR, Wong TY, Brancati FL, Hubbard LD, Couper D. ARIC Group. The association of atherosclerosis, vascular risk factors, and retinopathy in adults with diabetes : the atherosclerosis risk in communities study. Ophthalmology. 2002; 109:1225–1234.13. Rong J, Yu CQ, Yang P, Chen J. Association of retinopathy with coronary atherosclerosis determined by coronary 64-slice multidetector computed tomography angiography in type 2 diabetes. Diab Vasc Dis Res. 2013; 10:161–168.14. Johnson TR, Nikolaou K, Wintersperger BJ, Leber AW, von Ziegler F, Rist C, Buhmann S, Knez A, Reiser MF, Becker CR. Dual-source CT cardiac imaging: initial experience. Eur Radiol. 2006; 16:1409–1415.15. Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K, Shea S, Szklo M, Bluemke DA, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008; 358:1336–1345.16. American Diabetes Association. Nutrition recommendations and principles for people with diabetes mellitus. Diabetes Care. 2000; 23:Suppl 1. S43–6.17. Final report on the aspirin component of the ongoing Physicians’ Health Study. Steering Committee of the Physicians’ Health Study Research Group. N Engl J Med. 1989; 321:129–135.18. Puel J, Valensi P, Vanzetto G, Lassmann-Vague V, Monin JL, Moulin P, Ziccarelli C, Mayaudon H, Ovize M, Bernard S, et al. Identification of myocardial ischemia in the diabetic patient. Joint ALFEDIAM and SFC recommendations. Diabetes Metab. 2004; 30:3S3–3S18.19. Rydén L, Standl E, Bartnik M, Van den Berghe G, Betteridge J, de Boer MJ, Cosentino F, Jönsson B, Laakso M, Malmberg K, et al. Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD). Eur Heart J. 2007; 28:88–136.20. Cosson E, Nguyen MT, Chanu B, Balta S, Takbou K, Valensi P. The report of male gender and retinopathy status improves the current consensus guidelines for the screening of myocardial ischemia in asymptomatic type 2 diabetic patients. Nutr Metab Cardiovasc Dis. 2013; 23:557–565.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Biochemical Markers of Coronary Heart Disease Correlates Better to Metabolic Syndrome Defined by WHO than by NCEP-ATP III or IDF in Korean Type 2 Diabetic Patients
- The Biochemical Markers of Coronary Heart Disease Correlates Better to Metabolic Syndrome Defined by WHO than by NCEP-ATP III or IDF in Korean Type 2 Diabetic Patients
- The Relation of Microalbuminuria with Diabetic Retinopathy in Diabetic Patients without Proteinuria
- Clinical Analysis of Diabetic Retinopathy According to the Type of Diabetes Mellitus
- Factors Influencing the Level of Diabetic Retinopathy in Patients with Type 2 Diabetes Mellitus
