J Korean Med Sci.
2016 Jun;31(6):1003-1006. 10.3346/jkms.2016.31.6.1003.
Multiple Endocrine Neoplasia Type 1 Presenting as Hypoglycemia due to Insulinoma
- Affiliations
-
- 1Department of Pediatrics, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea.
- 2Department of Pediatrics, Masan Medical Center, Changwon, Korea.
- 3Department of Pediatrics, Hallym University College of Medicine, Seoul, Korea.
- 4Department of Pediatrics, Ajou University School of Medicine, Ajou University Hospital, Suwon, Korea. pedhwang@ajou.ac.kr
- KMID: 2373713
- DOI: http://doi.org/10.3346/jkms.2016.31.6.1003
Abstract
- Multiple endocrine neoplasia (MEN) mutation is an autosomal dominant disorder characterized by the occurrence of parathyroid, pancreatic islet, and anterior pituitary tumors. The incidence of insulinoma in MEN is relatively uncommon, and there have been a few cases of MEN manifested with insulinoma as the first symptom in children. We experienced a 9-year-old girl having a familial MEN1 mutation. She complained of dizziness, occasional palpitation, weakness, hunger, sweating, and generalized tonic-clonic seizure that lasted for 5 minutes early in the morning. At first, she was only diagnosed with insulinoma by abdominal magnetic resonance images of a 1.3 × 1.5 cm mass in the pancreas and high insulin levels in blood of the hepatic vein, but after her father was diagnosed with MEN1. We found she had familial MEN1 mutation, and she recovered hyperinsulinemic hypoglycemia after enucleation of the mass. Therefore, the early genetic identification of MEN1 mutation is considerable for children with at least one manifestation.
MeSH Terms
-
Alleles
Base Sequence
Child
DNA Mutational Analysis
Female
Humans
Hypoglycemia/diagnosis
Insulin/blood
Insulinoma/diagnostic imaging/*pathology
Magnetic Resonance Imaging
Multiple Endocrine Neoplasia Type 1/*diagnosis/pathology
Pancreatic Neoplasms/diagnostic imaging/*pathology
Pedigree
Polymorphism, Single Nucleotide
Proto-Oncogene Proteins/genetics
Seizures/complications
Insulin
Proto-Oncogene Proteins
Figure
-
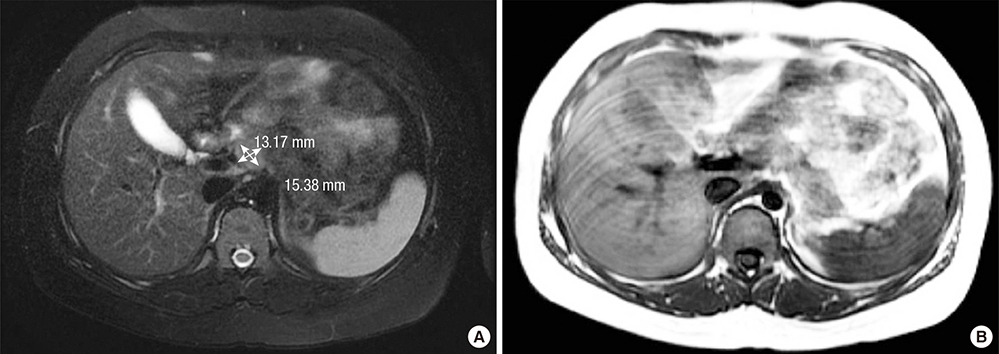
Fig. 1 MR study of the pancreas. (A) A mass with hyposignal intensity on T1 weighted images, 1.3 × 1.5 cm. (B) High signal intensity on T2 weighted images at the head of the pancreas.
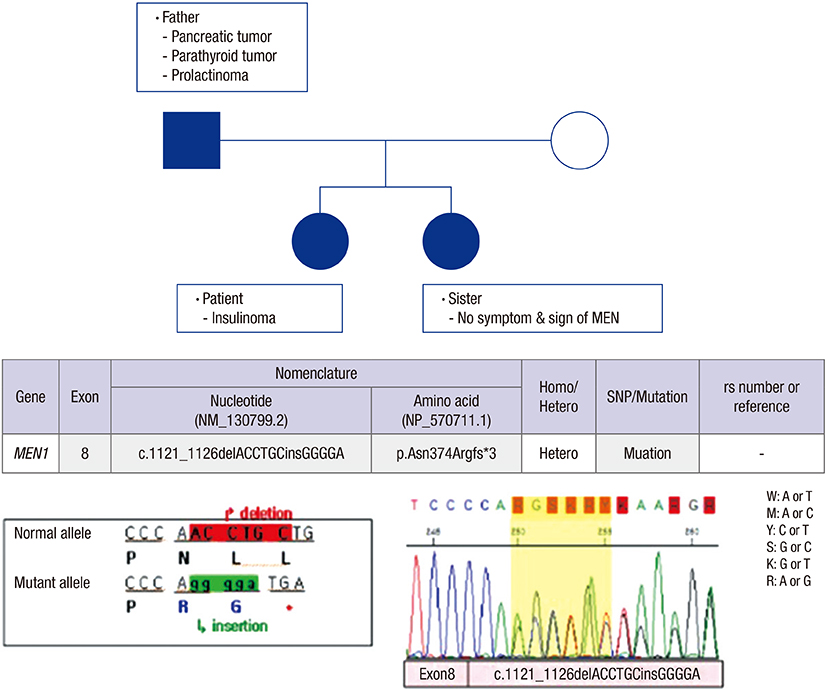
Fig. 2 Pedigree and DNA sequencing analysis. MEN 1 mutation. (c.1121_1126delACCTGCinsGGGGA) was found in the patient, patient's father and younger sister.
Reference
-
1. LaFranchi S. Hypoglycemia of infancy and childhood. Pediatr Clin North Am. 1987; 34:961–982.2. Okabayashi T, Shima Y, Sumiyoshi T, Kozuki A, Ito S, Ogawa Y, Kobayashi M, Hanazaki K. Diagnosis and management of insulinoma. World J Gastroenterol. 2013; 19:829–837.3. Iglesias P, Díez JJ. Management of endocrine disease: a clinical update on tumor-induced hypoglycemia. Eur J Endocrinol. 2014; 170:R147–57.4. Thakker RV, Newey PJ, Walls GV, Bilezikian J, Dralle H, Ebeling PR, Melmed S, Sakurai A, Tonelli F, Brandi ML. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J Clin Endocrinol Metab. 2012; 97:2990–3011.5. Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, Service FJ. Endocrine Society. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009; 94:709–728.6. Placzkowski KA, Vella A, Thompson GB, Grant CS, Reading CC, Charboneau JW, Andrews JC, Lloyd RV, Service FJ. Secular trends in the presentation and management of functioning insulinoma at the Mayo Clinic, 1987-2007. J Clin Endocrinol Metab. 2009; 94:1069–1073.7. Service FJ, McMahon MM, O’Brien PC, Ballard DJ. Functioning insulinoma--incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991; 66:711–719.8. Machens A, Schaaf L, Karges W, Frank-Raue K, Bartsch DK, Rothmund M, Schneyer U, Goretzki P, Raue F, Dralle H. Age-related penetrance of endocrine tumours in multiple endocrine neoplasia type 1 (MEN1): a multicentre study of 258 gene carriers. Clin Endocrinol (Oxf). 2007; 67:613–622.9. Marini F, Falchetti A, Del Monte F, Carbonell Sala S, Gozzini A, Luzi E, Brandi ML. Multiple endocrine neoplasia type 1. Orphanet J Rare Dis. 2006; 1:38.10. Thakker RV. Multiple endocrine neoplasia type 1 (MEN1) and type 4 (MEN4). Mol Cell Endocrinol. 2014; 386:2–15.11. Trump D, Farren B, Wooding C, Pang JT, Besser GM, Buchanan KD, Edwards CR, Heath DA, Jackson CE, Jansen S, et al. Clinical studies of multiple endocrine neoplasia type 1 (MEN1). QJM. 1996; 89:653–669.12. Bassett JH, Forbes SA, Pannett AA, Lloyd SE, Christie PT, Wooding C, Harding B, Besser GM, Edwards CR, Monson JP, et al. Characterization of mutations in patients with multiple endocrine neoplasia type 1. Am J Hum Genet. 1998; 62:232–244.13. Turner JJ, Christie PT, Pearce SH, Turnpenny PD, Thakker RV. Diagnostic challenges due to phenocopies: lessons from Multiple Endocrine Neoplasia type1 (MEN1). Hum Mutat. 2010; 31:E1089–101.14. de Vogelaere K, De Schepper J, Vanhoeij M, De Mey J, Goossens A, Vanbesien J, De Backer A, Delvaux G. Laparoscopic management of insulinoma in a child with multiple endocrine neoplasia type 1. J Laparoendosc Adv Surg Tech A. 2006; 16:335–338.15. Winston KY, Dawrant J. A rare case of hypoglycaemia due to insulinoma in an adolescent with acutely altered mental status. J Pediatr Endocrinol Metab. 2014; 27:773–776.16. Panamonta O, Areemit S, Srinakarin J, Puapairoj A. Insulinoma in childhood. J Med Assoc Thai. 2001; 84:136–142.17. Janem W, Sultan I, Ajlouni F, Deebajeh R, Haddad H, Sughayer MA, Goussous RY. Malignant insulinoma in a child. Pediatr Blood Cancer. 2010; 55:1423–1426.18. Akerström G, Hellman P. Surgery on neuroendocrine tumours. Best Pract Res Clin Endocrinol Metab. 2007; 21:87–109.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Insulinoma Combined with Pheochromocytoma
- A Novel Germline Mutation of MEN1 Gene in a Young-aged Multiple Insulinoma with Hyperparathyroidism
- A Case of Multiple Endocrine Neoplasia Type 1 with Primary Liver Gastrinoma
- Familial Multiple Endocrine Neoplasia, Type I, in Identical Twins
- A Case of Multiple Endocrine Neoplasia Type 1
