A Case of Primary Gastric Amyloidosis with Fulminant Heart Failure
- Affiliations
-
- 1Department of Internal Medicine, Kyung Hee University School of Medicine, Seoul, Korea. cywgi@chol.com
- 2Department of Pathology, Kyung Hee University School of Medicine, Seoul, Korea.
- KMID: 2373346
- DOI: http://doi.org/10.4166/kjg.2015.66.4.227
Abstract
- A 53-year-old woman was admitted with epigastric discomfort and weakness. Laboratory examination at admission showed mild anemia and proteinuria. Esophagogastroduodenoscopy revealed marked mucosal atrophy, diffuse nodularity and granular appearance with mucosal friability. Biopsy was performed on the antrum and body of the stomach. On the next day, the patient began to complain of severe dyspnea, and hypoxia was present on pulse oximetry. Therefore, emergency echocardiography was conducted and it showed restrictive cardiomyopathy along with thrombus in the left atrium. With time, heart failure was aggravated despite intensive management. The result of gastric biopsy revealed amyloid deposits which stained positively with Congo red. On immunohistochemistry study, kappa and lambda chain were present. In addition, kappa chain was significantly elevated in urine and serum on electrophoresis. Although the patient was finally diagnosed as having primary gastric amyloidosis with restrictive cardiomyopathy, her general condition rapidly deteriorated and died at 12th hospital day. When obscure gastric lesion is encountered, performing gastric biopsy is strongly recommended since it be primary gastric amyloidosis. Herein, we present an unusual case of primary gastric amyloidosis.
Keyword
MeSH Terms
-
Amyloidosis/complications/*diagnosis/pathology
Endoscopy, Digestive System
Female
Heart Atria/diagnostic imaging
Heart Failure/complications/*diagnosis
Humans
Immunoglobulin kappa-Chains/blood/urine
Immunoglobulin lambda-Chains/blood/urine
Immunohistochemistry
Magnetic Resonance Imaging
Middle Aged
Stomach Diseases/complications/*diagnosis/pathology
Thrombosis/diagnosis/diagnostic imaging
Tomography, X-Ray Computed
Ultrasonography
Immunoglobulin kappa-Chains
Immunoglobulin lambda-Chains
Figure
-
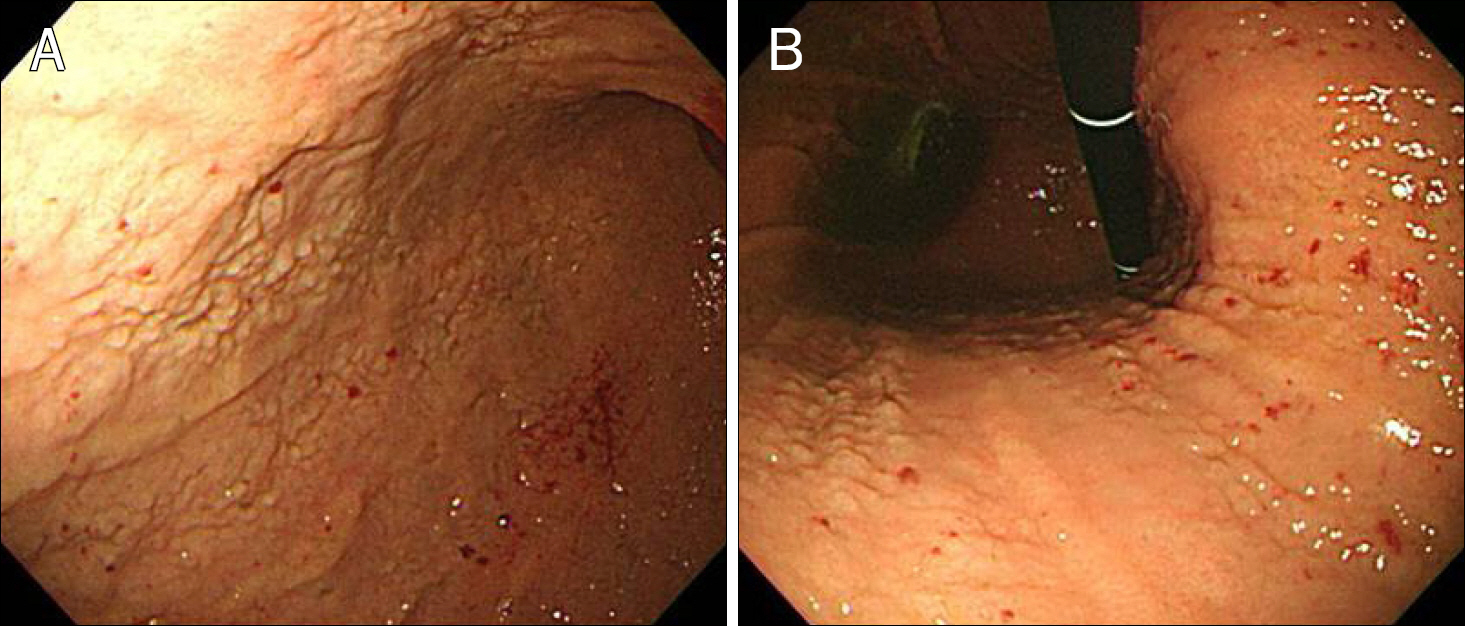
Fig. 1. Endoscopic findings of the stomach. (A) On greater curvature and (B) lesser curvature of the stomach, marked mucosal atrophy and diffuse granular surface appearances are noted along with mucosal friability.
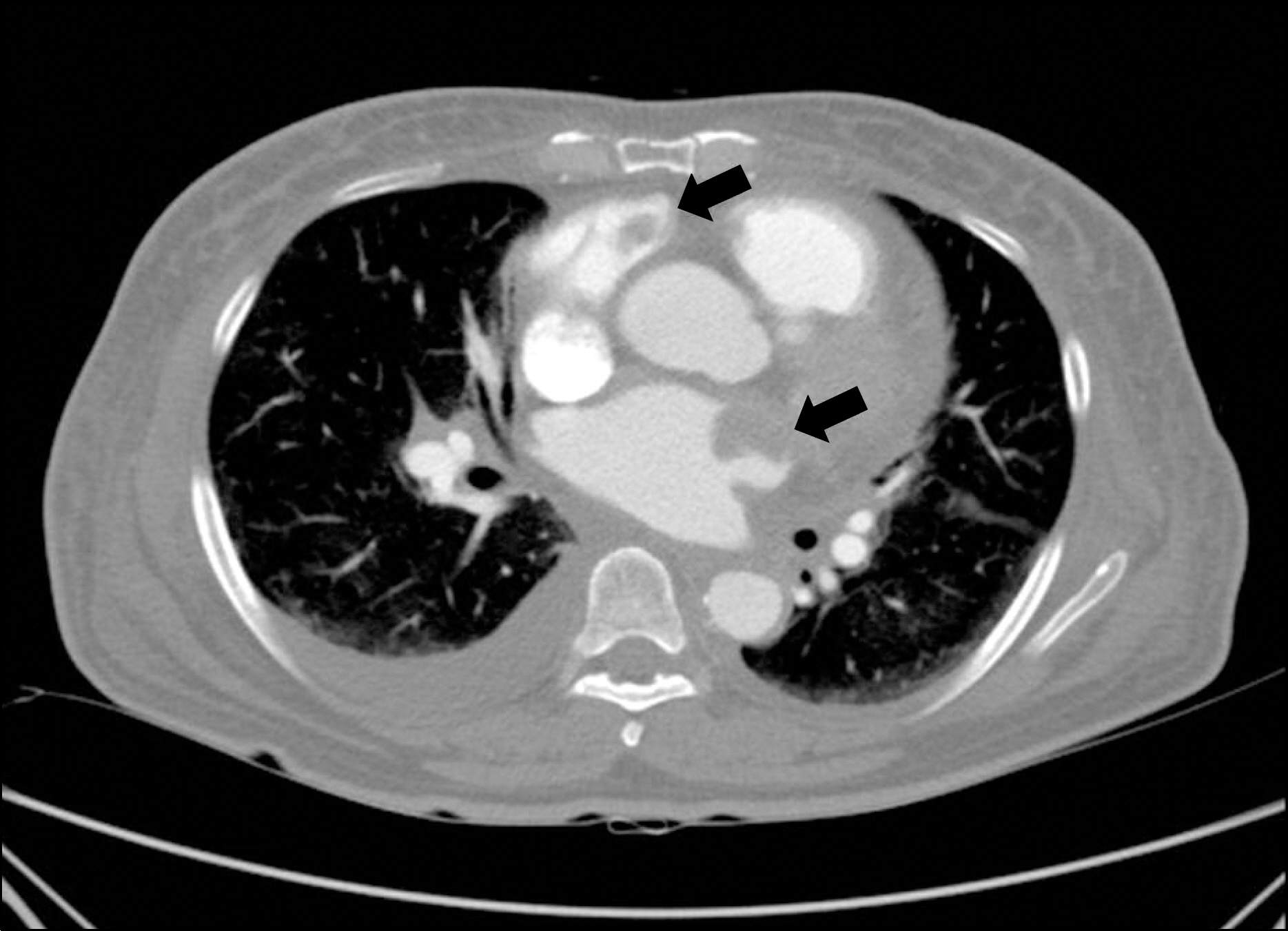
Fig. 2. CT scan of the thorax. Two thrombi are present in the right atrium and left atrium appendage (arrows). Pleural effusion is also observed.

Fig. 3. Echocardiography. Significant hypertrophy and bright twinkling echogenecity are observed. A thrombus is also noted in the left atrium (arrow).
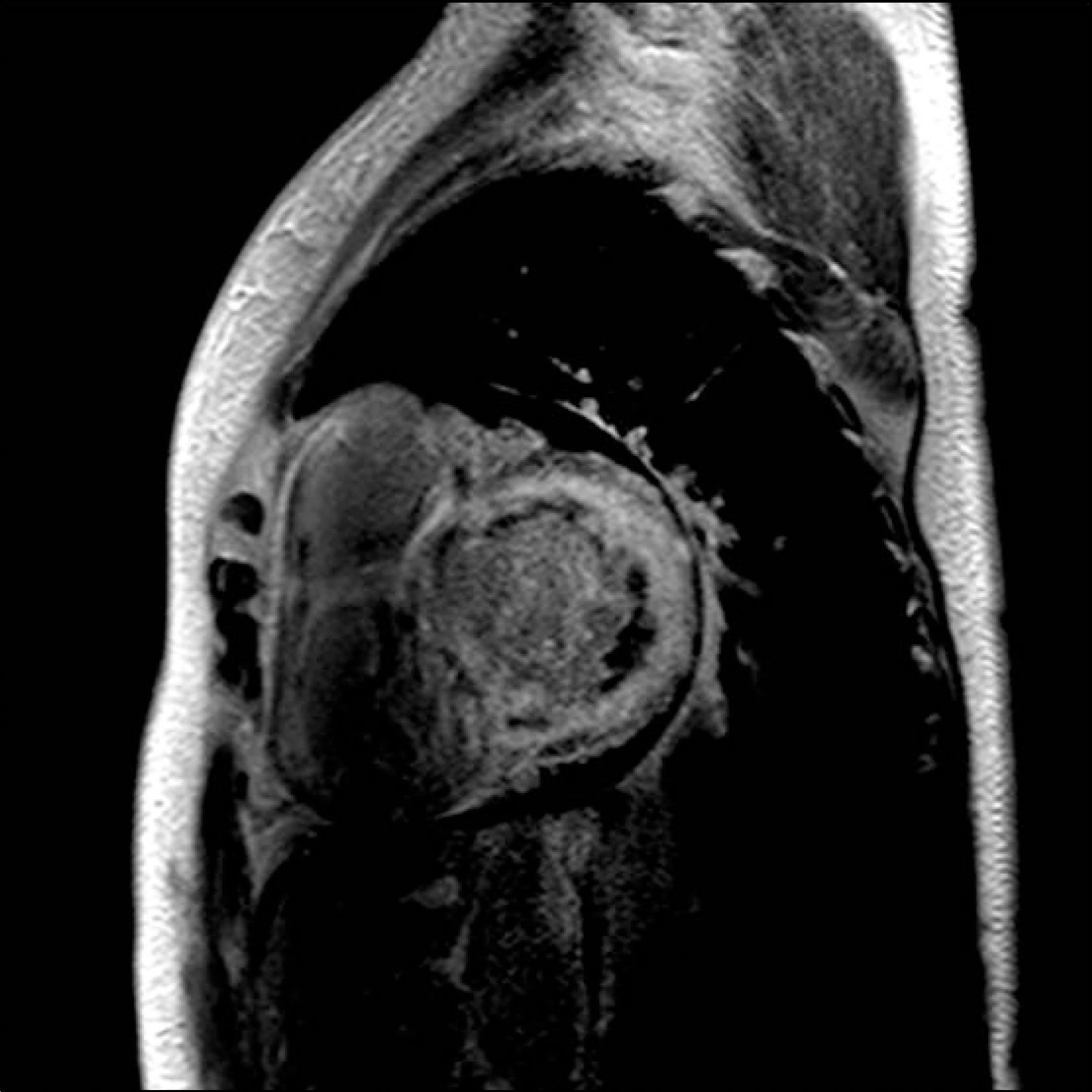
Fig. 4. Cardiac MRI. On delayed enhanced image, abnormal global subendocardial enhancement is shown.
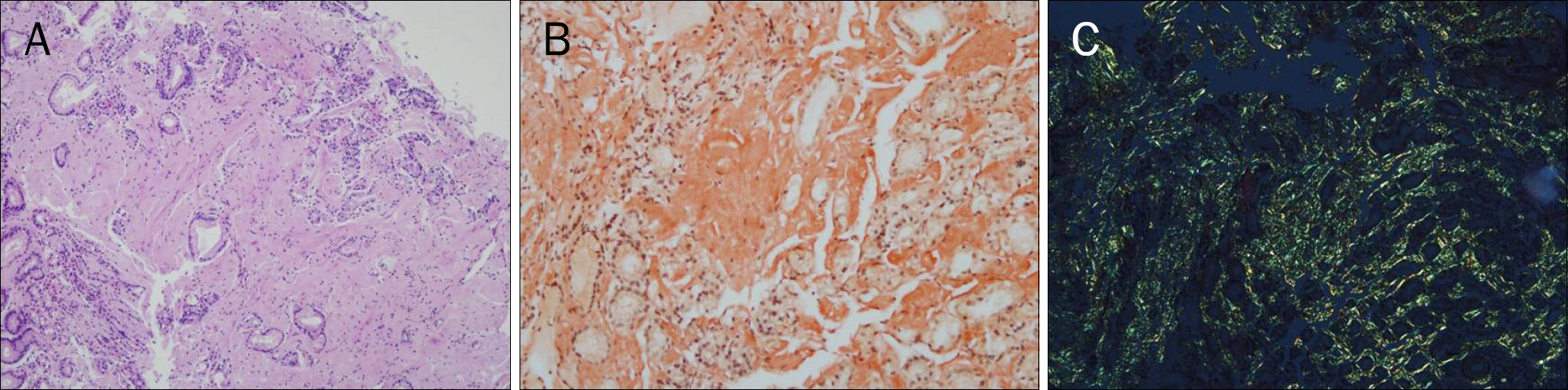
Fig. 5. Microscopic findings. (A) Profound eosinophilic masses are noted in lamina propria (H&E, ×100). (B) Congo-red stain reveals pink red deposits (×200). (C) The yellow-green bifringence of the deposits is observed by polarizing microscope (×200).
Reference
-
References
1. Merlini G, Comenzo RL, Seldin DC, Wechalekar A, Gertz MA. Immunoglobulin light chain amyloidosis. Expert Rev Hematol. 2014; 7:143–156.
Article2. Kyle RA, Gertz MA. Primary systemic amyloidosis: clinical and laboratory features in 474 cases. Semin Hematol. 1995; 32:45–59.3. Menke DM, Kyle RA, Fleming CR, Wolfe JT 3rd, Kurtin PJ, Oldenburg WA. Symptomatic gastric amyloidosis in patients with primary systemic amyloidosis. Mayo Clin Proc. 1993; 68:763–767.
Article4. Kim YJ, Kim HS, Park SY, et al. Intestinal amyloidosis with intractable diarrhea and intestinal pseudoobstruction. Korean J Gastroenterol. 2012; 60:172–176.
Article5. Kwon YH, Kim JY, Kim JH, et al. A case of primary colon amyloidosis presenting as hematochezia. Korean J Gastroenterol. 2012; 59:44–47.
Article6. Park SW, Lee HW, Cho EJ. Systemic amyloidosis manifested by gastric outlet obstruction. Clin Endosc. 2013; 46:579–581.
Article7. Tada S, Iida M, Iwashita A, et al. Endoscopic and biopsy findings of the upper digestive tract in patients with amyloidosis. Gastrointest Endosc. 1990; 36:10–14.
Article8. Said SM, Grogg KL, Smyrk TC. Gastric amyloidosis: clinicopathological correlations in 79 cases from a single institution. Hum Pathol. 2015; 46:491–498.
Article9. Lee YN, Hong SJ, Kim HK. Localized gastric amyloidosis. Korean J Gastroenterol. 2011; 58:117–120.
Article10. Dubrey SW, Hawkins PN, Falk RH. Amyloid diseases of the heart: assessment, diagnosis, and referral. Heart. 2011; 97:75–84.
Article11. Feng D, Edwards WD, Oh JK, et al. Intracardiac thrombosis and embolism in patients with cardiac amyloidosis. Circulation. 2007; 116:2420–2426.
Article12. Comenzo RL, Reece D, Palladini G, et al. Consensus guidelines for the conduct and reporting of clinical trials in systemic light-chain amyloidosis. Leukemia. 2012; 26:2317–2325.
Article13. Palladini G, Milani P, Foli A, et al. Oral melphalan and dexamethasone grants extended survival with minimal toxicity in AL amyloidosis: long-term results of a risk-adapted approach. Haematologica. 2014; 99:743–750.
Article14. Mikhael JR, Schuster SR, Jimenez-Zepeda VH, et al. Cyclopho-sphamide-bortezomib-dexamethasone (CyBorD) produces rapid and complete hematologic response in patients with AL amyloidosis. Blood. 2012; 119:4391–4394.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Primary Renal Amyloidosis with Fulminant Hepatic Failure
- A Case of Systemic Amyloidosis
- A Case of Multiple Myeloma of Kappa Light Chain Type Associated with Gastric Amyloidosis and Acute Renal Failure and Pathologic Fracture Due to Femur Plasmacytoma
- A Patient with Primary Amyloidosis Misrecognized as Thyrotoxicosis-induced Heart Failure
- A Case of Primary Systemic Amyloidosis Predominantly Presenting Nephrotic Syndrome and Peripheral Neuropathy
