A Case of Cavernous Lymphangioma of the Small Bowel Mesentery
- Affiliations
-
- 1Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea. drcha@khu.ac.kr
- KMID: 2373335
- DOI: http://doi.org/10.4166/kjg.2015.66.3.172
Abstract
- Lymphangioma is a benign vascular lesion with characteristics of subepithelial tumor which can proliferate in the lymphatic system. Lymphangioma of the small-bowel mesentery is rare, having been reported in less than 2% of all lymphangiomas. Lymphangioma does not require any specific treatment because it is absolutely a benign tumor. However, surgical exploration is rarely required for cases with disease-related symptoms or complications, or for those misdiagnosed as a malignant lesion. We recently experienced a case of mesenteric cavernous lymphangomas in a 53-year-old female who was misdiagnosed as having a liposarcoma. The final diagnosis was confirmed by a pathologic examination of the specimen that was obtained via laparoscopic exploration. Herein, we report a very rare case of mesenteric cavernous lymphangioma along with a brief review of relevant literature.
Keyword
MeSH Terms
Figure
-

Fig. 1. Abdominal CT findings. (A) Initial CT shows 1.3 cm sized soft tissue mass (arrow) in small bowel mesentery. (B) Follow-up CT shows increased size of the lesions from 1.3 to 2 cm (arrowheads) compared with previous CT scan performed 7 months ago.

Fig. 2. Laparoscopic exploration demonstrates mesenteric fat thickening and cystic mass.
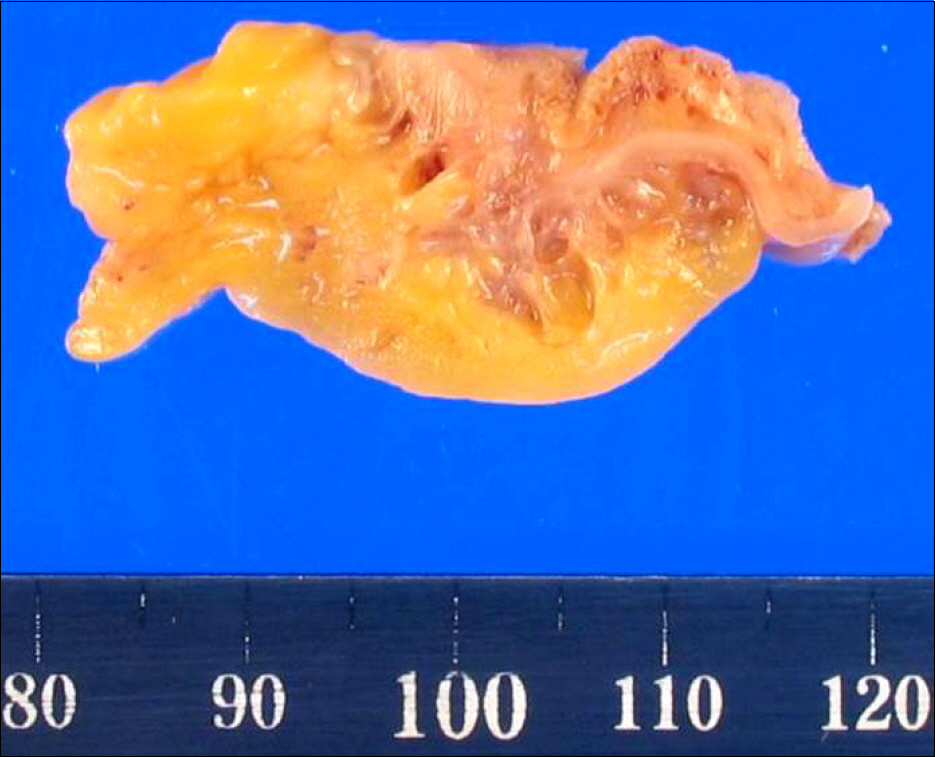
Fig. 3. Gross finding of resected specimen. Gross pathologic examination reveals a 3.5×1.5×1.2 cm sized mass composed of various- sized cysts.

Fig. 4. Microscopic findings. (A) There are many dilated lymphatic vessels lined by a single layer of endothelium (H&E, ×40). (B) Dilated lymphatic vessels are filled with proteinaceous fluid (H&E, ×100). (C) The lining cells are positive for D2–40 (immunohistochemical stain, ×100).
Reference
-
References
1. Fonkalsrud EW. Congenital malformations of the lymphatic system. Semin Pediatr Surg. 1994; 3:62–69.2. Tsukada H, Takaori K, Ishiguro S, Tsuda T, Ota S, Yamamoto T. Giant cystic lymphangioma of the small bowel mesentery: report of a case. Surg Today. 2002; 32:734–737.
Article3. Mosca RC, Pereira GA, Mantesso A. Cystic hygroma: characterization by computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:e65–e69.
Article4. Hanagiri T, Baba M, Shimabukuro T, et al. Lymphangioma in the small intestine: report of a case and review of the Japanese literature. Surg Today. 1992; 22:363–367.
Article5. Na WT, Lee TH, Lee BS, et al. Clinical aspects of intraabdominal cystic lymphangioma in Korea. Korean J Gastroenterol. 2010; 56:353–358.
Article6. Batsakis JG. Tumors of the head and neck: clinical and pathological consideration. Volume 1. 2nd ed.Baltimore: Williams & Wilkins;1979. p. 301–302.7. Chung JH, Suh YL, Park IA, et al. A pathologic study of abdominal lymphangiomas. J Korean Med Sci. 1999; 14:257–262.
Article8. Kahn HJ, Bailey D, Marks A. Monoclonal antibody D2–40, a new marker of lymphatic endothelium, reacts with Kaposi's sarcoma and a subset of angiosarcomas. Mod Pathol. 2002; 15:434–440.
Article9. Jeung MY, Gasser B, Gangi A, et al. Imaging of cystic masses of the mediastinum. Radiographics. 2002; 22(Suppl 1):S79–S93.
Article10. Vargas-Serrano B, Alegre-Bernal N, Cortina-Moreno B, Rodriguez- Romero R, Sanchez-Ortega F. Abdominal cystic lymphangiomas: US and CT findings. Eur J Radiol. 1995; 19:183–187.
Article11. Kim HH, Hur YH, Park CY, et al. Splenic cavernous lymphangioma mimicking splenic hemangioma. J Korean Surg Soc. 2009; 77:434–437.
Article12. Hwang SS, Choi HJ, Park SY. Cavernous mesenteric lymphangiomatosis mimicking metastasis in a patient with rectal cancer: a case report. World J Gastroenterol. 2009; 15:3947–3949.
Article13. Iyer R, Eftekhari F, Varma D, Jaffe N. Cystic retroperitoneal lymphangioma: CT, ultrasound and MR findings. Pediatr Radiol. 1993; 23:305–306.
Article14. Beneck D, Abati AD, Greco MA. Lymphangioma presenting as a nasal polyp in an infant. Arch Pathol Lab Med. 1985; 109:773–775.15. Price C. Cystic lymphangioma in the maxillary sinus: a case report. Br J Oral Surg. 1976; 14:41–46.
Article16. Chung WC, Kim HK, Yoo JY, et al. Colonic lymphangiomatosis associated with anemia. World J Gastroenterol. 2008; 14:5760–5762.
Article17. Lee JH, Lee SY, Lee JH, et al. A case of colonic intussusception caused by cystic lymphangioma of the colon. Korean J Gastrointest Endosc. 2006; 32:226–230.18. Ha CY, Shim KN, Kang MJ, et al. A case of cystic lymphangioma of small bowel mesentery presented with small bowel volvulus. Intest Res. 2008; 6:76–79.19. Saba C, Bossi MC, Barletta A. Therapy of subcutaneous cystic lymphangioma with ultrasound-guided puncture and alcoholi-zation. Radiol Med. 1992; 83:270–272.20. Okada A, Kubota A, Fukuzawa M, Imura K, Kamata S. Injection of bleomycin as a primary therapy of cystic lymphangioma. J Pediatr Surg. 1992; 27:440–443.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cavernous lymphangioma of the ileal mesentery: A case report
- A Case of Cystic Lymphangioma of Small Bowel Mesentery Presented with Small Bowel Volvulus
- Cystic Lymphangioma Involving the Mesentery and the Retroperitoneum: A Case Report
- A Rare Case of Large Hemolymphangioma in the Small Bowel Mesentery : A Case Report
- Fat containing chylous mesenteric lymphangiomatosis
