A Pyloric Gland-Phenotype Ovarian Mucinous Tumor Resembling Lobular Endocervical Glandular Hyperplasia in a Patient with Peutz-Jeghers Syndrome
- Affiliations
-
- 1Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. krkim@amc.seoul.kr
- 2Department of Medical Genetics, Asan Medical Center Children’s Hospital, Seoul, Korea.
- KMID: 2372965
- DOI: http://doi.org/10.4132/jptm.2016.07.01
Abstract
- We describe an ovarian mucinous neoplasm that histologically resembles lobular endocervical glandular hyperplasia (LEGH) containing pyloric gland type mucin in a patient with Peutz-Jeghers syndrome (PJS). Although ovarian mucinous tumors rarely occur in PJS patients, their pyloric gland phenotype has not been clearly determined. The histopathologic features of the ovarian mucinous tumor were reminiscent of LEGH. The cytoplasmic mucin was stained with periodic acid-Schiff reaction after diastase treatment but was negative for Alcian blue pH 2.5, suggesting the presence of neutral mucin. Immunohistochemically, the epithelium expressed various gastric markers, including MUC6, HIK1083, and carbonic anhydrase-IX. Multiple ligation-dependent probe amplification detected a germline heterozygous deletion mutation at exons 1-7 of the STK11 gene (c.1-?_920+?del) in peripheral blood leukocytes and mosaic loss of heterozygosity in ovarian tumor tissue. Considering that LEGH and/or gastric-type cervical adenocarcinoma can be found in patients with PJS carrying germline and/or somatic STK11 mutations, our case indicates that STK11 mutations have an important role in the proliferation of pyloric-phenotype mucinous epithelium at various anatomical locations.
Keyword
Figure
-
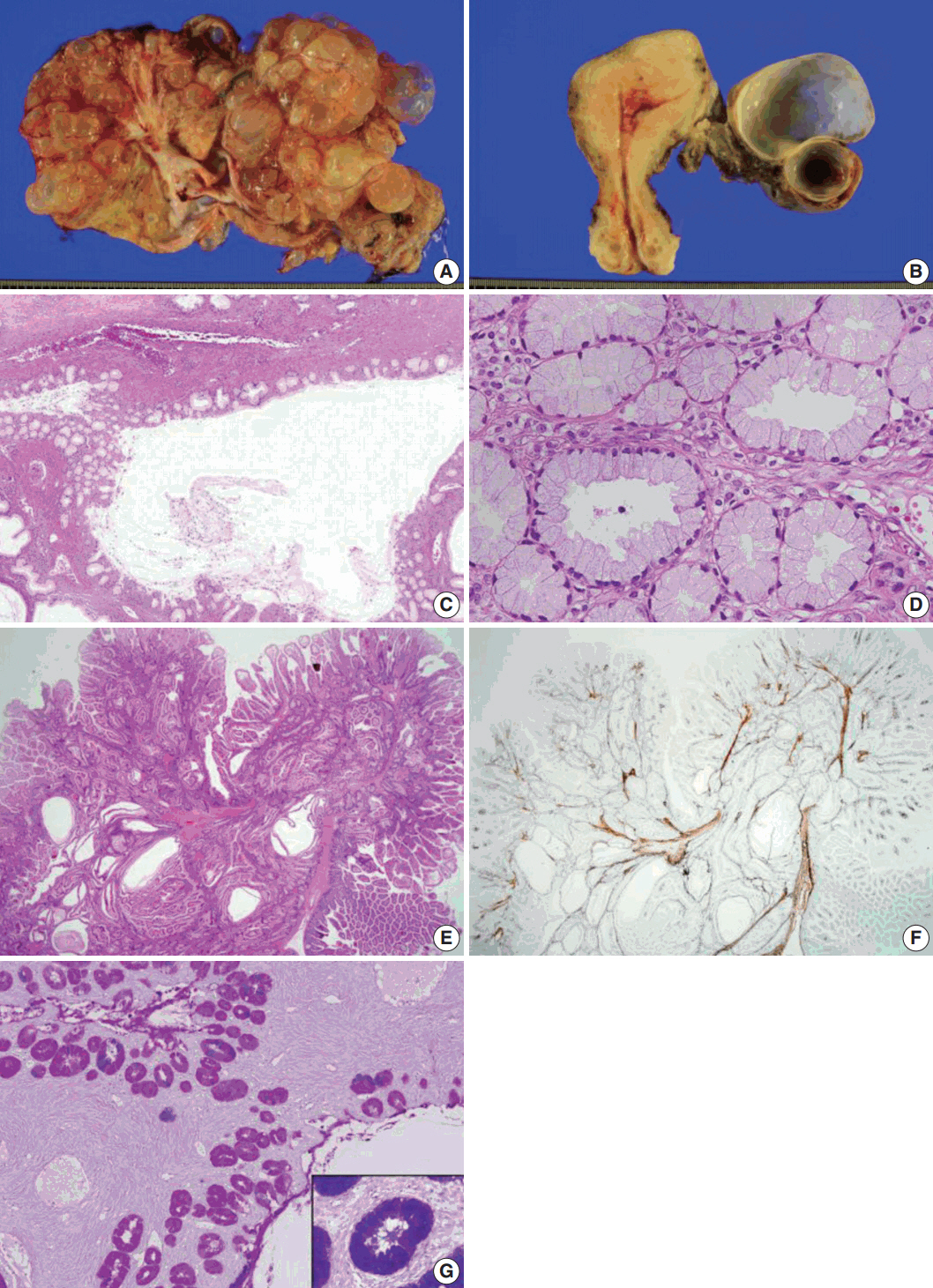
Fig. 1. Sectioned surface of the left ovary showing multilocular cysts filled with mucinous fluid (A) and the cut surface of the right ovary (B). No apparent abnormality is identified on the surface of the uterine cervix and endometrium. Microscopically, the ovarian mucinous tumor is composed of a large dilated duct-like structure with clusters of small glands, reminiscent of lobular endocervical glandular hyperplasia of the uterine cervix (C). At higher magnification, the cysts are lined by a single layer of mucinous epithelium with bland nuclei and pale eosinophilic cytoplasm. Stratification or mitosis is not identified (D). The small bowel polyps in this patient show hyperplastic mucosa with arborizing strands of smooth muscle in various directions (E), highlighted by desmin immunostaining (F). Combined Alcian blue pH 2.5 and periodic acid-Schiff stains after diastase treatment show bright pink-colored cytoplasm, indicating predominant neutral mucin in the cytoplasm of the ovarian mucinous epithelium (G) in contrast to the purple-violet color in normal endocervical epithelium (G, inlet).
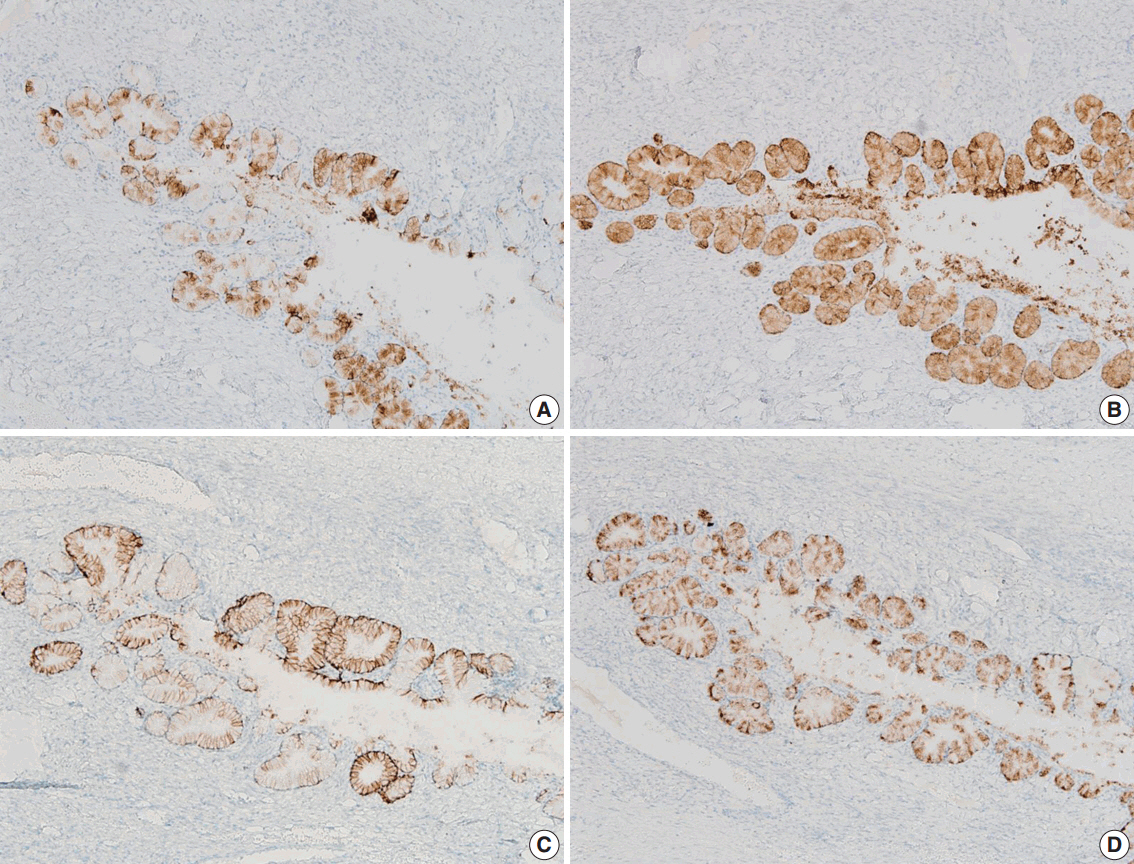
Fig. 2. The mucinous epithelium of the ovary shows immunoreactivity for various gastric markers, including MUC5AC (A), MUC6 (B), carbonic anhydrase-IX (C), and HIK1083 (D), indicating the gastric phenotype of the mucinous epithelium.
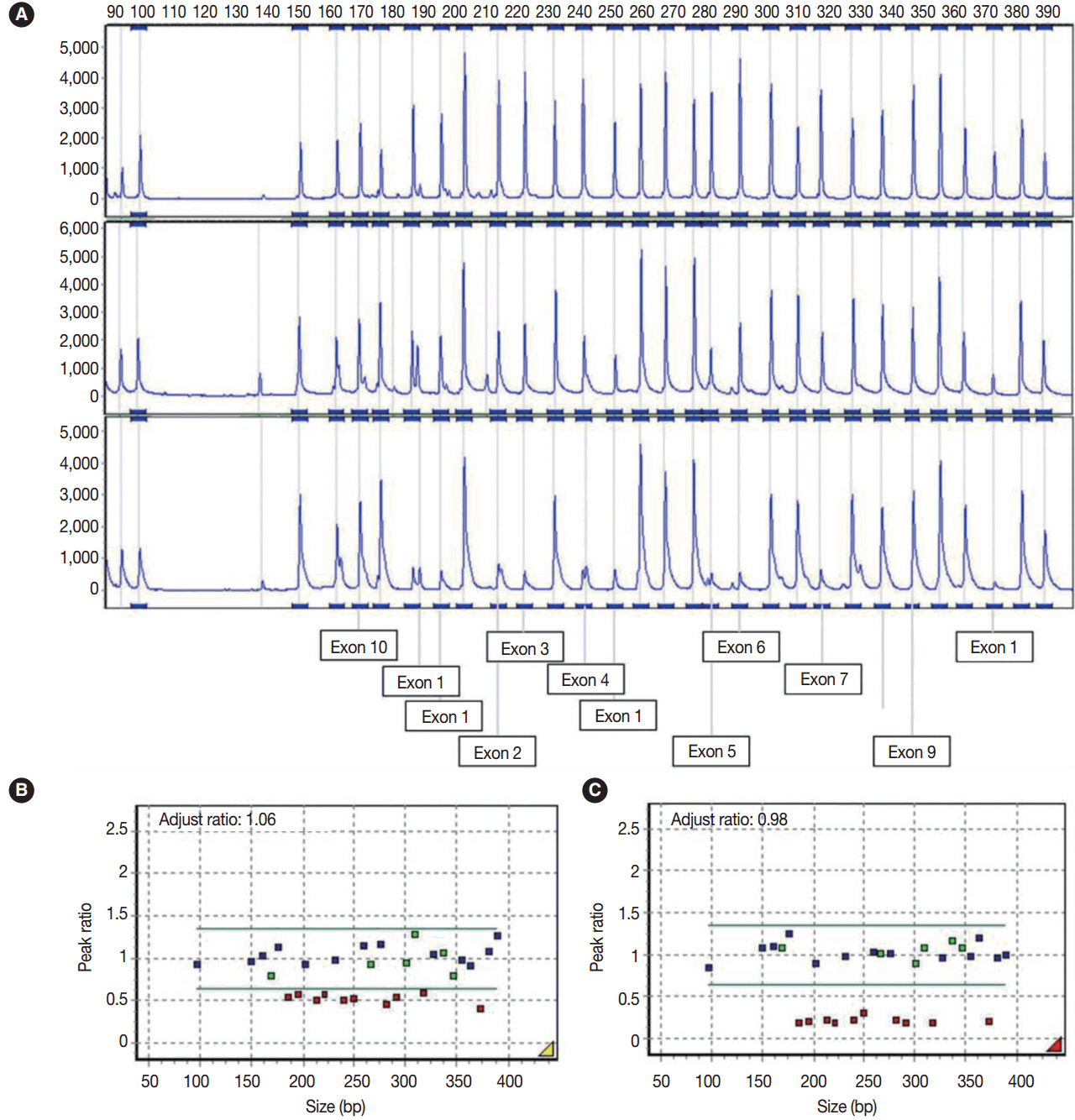
Fig. 3. (A) Electrogram showing multiple ligation-dependent probe amplification analysis of the STK11 gene. The X-axis indicates product size (bp) and the Y-axis indicates the fluorescence intensities as the dosage of the products. The exon numbers of STK11 are marked below the electrogram. The peaks are those of a normal control (A, upper), peripheral blood leukocyte (A, middle), and left ovarian mucinous cystadenoma (A, lower). (B) In the peripheral blood leukocytes, a peak ratio less than 0.65 represented the deletion mutation in the STK11 gene. (C) Ovarian mucinous tumor with lobular endocervical glandular hyperplasia-like features showing mosaic loss of heterozygosity on mutation analysis (heteroplasmy) through exon 1 to 7 with a peak ratio of about 0.25. The X-axis indicates product size (bp) and the Y-axis represents the adjusted peak ratios with normal controls. The adjusted ratio was standardized to the control sample, and the median point was considered to be 1.0.
Reference
-
1. Ferry JA, Young RH, Engel G, Scully RE. Oxyphilic Sertoli cell tumor of the ovary: a report of three cases, two in patients with the Peutz-Jeghers syndrome. Int J Gynecol Pathol. 1994; 13:259–66.
Article2. Jenne DE, Reimann H, Nezu J, et al. Peutz-Jeghers syndrome is caused by mutations in a novel serine threonine kinase. Nat Genet. 1998; 18:38–43.3. Kuragaki C, Enomoto T, Ueno Y, et al. Mutations in the STK11 gene characterize minimal deviation adenocarcinoma of the uterine cervix. Lab Invest. 2003; 83:35–45.
Article4. Kato N, Sugawara M, Maeda K, Hosoya N, Motoyama T. Pyloric gland metaplasia/differentiation in multiple organ systems in a patient with Peutz-Jegher’s syndrome. Pathol Int. 2011; 61:369–72.
Article5. Kondo T, Hashi A, Murata S, et al. Endocervical adenocarcinomas associated with lobular endocervical glandular hyperplasia: a report of four cases with histochemical and immunohistochemical analyses. Mod Pathol. 2005; 18:1199–210.
Article
