J Gastric Cancer.
2010 Dec;10(4):241-246.
The Early Experience of Laparoscopy-assisted Gastrectomy for Gastric Cancer at a Low-volume Center
- Affiliations
-
- 1Department of Surgery, National Medical Center, Seoul, Korea. jmparkgs@gmail.com
Abstract
- PURPOSE
Laparoscopy-assisted gastrectomy (LAG) has become a technically feasible and safe procedure for early gastric cancer treatment. LAG is being increasingly performed in many centers; however, there have been few reports regarding LAG at low-volume centers. The aim of this study was to report our early experience with LAG in patients with gastric cancer at a low-volume center.
MATERIALS AND METHODS
The clinicopathologic data and surgical outcomes of 39 patients who underwent LAG for gastric cancer between April 2007 and March 2010 were retrospectively reviewed.
RESULTS
The mean age was 68.3 years. Thirty-one patients had medical co-morbidities. The mean patient ASA score was 2.0. Among the 39 patients, 4 patients underwent total gastrectomies and 35 patients underwent distal gastrectomies. The mean blood loss was 145.4 ml and the mean operative time was 259.4 minutes. The mean time-to-first flatus, first oral intake, and the postoperative hospital stay was 2.8, 3.1, and 9.3 days, respectively. The 30-day mortality rate was 0%. Postoperative complications developed in 9 patients, as follows: anastomotic leakage, 1; wound infection, 1; gastric stasis, 2; postoperative ileus, 1; pneumonia, 1; cerebral infarction, 1; chronic renal failure, 1; and postoperative psychosis, 1.
CONCLUSIONS
LAG is technically feasible and can be performed safely at a low-volume center, but an experienced surgical team and careful patient selection are necessary. Furthermore, for early mastery of the learning curve for LAG, surgeons need education and training in addition to an accumulation of cases.
Keyword
MeSH Terms
Figure
-
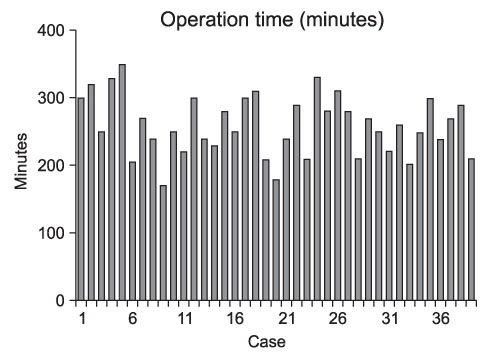
Fig. 1 Operative time of the each case.
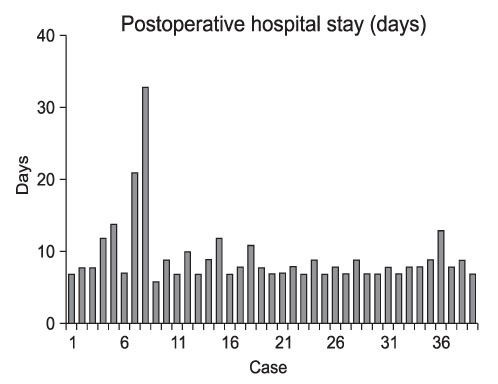
Fig. 2 Postoperative hospital stay of the each case.
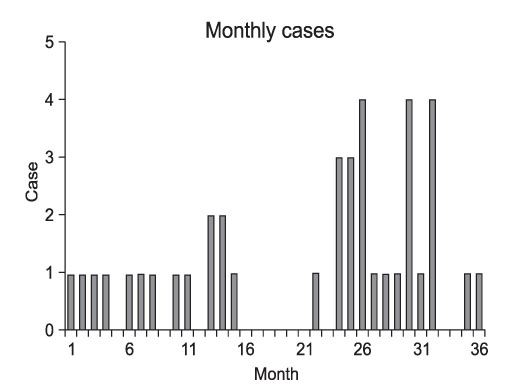
Fig. 3 The numbers of operations per month.
Reference
-
1. Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N. Japanese Laparoscopic Surgery Study Group. A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg. 2007. 245:68–72.
Article2. Azagra JS, Goergen M, De Simone P, Ibanez-Aguirre J. The current role of laparoscopic surgery in the treatment of benign gastroduodenal diseases. Hepatogastroenterology. 1999. 46:1522–1526.3. Adachi Y, Suematsu T, Shiraishi N, Katsuta T, Morimoto A, Kitano S, et al. Quality of life after laparoscopy-assisted Billroth I gastrectomy. Ann Surg. 1999. 229:49–54.
Article4. Keats AS. The ASA classification of physical status--a recapitulation. Anesthesiology. 1978. 49:233–236.
Article5. Korea Gastric Cancer Association. Nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2002. 2:105–114.6. Lee CH, Lee SI, Ryu KW, Mok YJ. Chronological changes in the clinical features of gastric cancer. J Korean Gastric Cancer Assoc. 2001. 1:161–167.
Article7. Hyung WJ, Cheong JH, Kim J, Chen J, Choi SH, Noh SH. Analysis of prognostic factors and gastric cancer specific survival rate in early gastric cancer patients and its clinical implication. J Korean Surg Soc. 2003. 65:309–315.8. Japanese Gastric Cancer Association Registration Committee. Maruyama K, Kaminishi M, Hayashi K, Isobe Y, Honda I, Katai H, et al. Gastric cancer treated in 1991 in Japan: data analysis of nationwide registry. Gastric Cancer. 2006. 9:51–66.
Article9. Kim MC, Jung GJ, Kim HH. Learning curve of laparoscopy-assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer. World J Gastroenterol. 2005. 11:7508–7511.
Article10. Zhang X, Tanigawa N. Learning curve of laparoscopic surgery for gastric cancer, a laparoscopic distal gastrectomy-based analysis. Surg Endosc. 2009. 23:1259–1264.
Article11. Jin SH, Kim DY, Kim H, Jeong IH, Kim MW, Cho YK, et al. Multidimensional learning curve in laparoscopy-assisted gastrectomy for early gastric cancer. Surg Endosc. 2007. 21:28–33.
Article12. Park JM, Jin SH, Lee SR, Kim H, Jung IH, Cho YK, et al. Complications with laparoscopically assisted gastrectomy: multivariate analysis of 300 consecutive cases. Surg Endosc. 2008. 22:2133–2139.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopy-Assisted Distal Gastrectomy for Early Gastric Cancer in the Elderly
- Comparison of Laparoscopy-Assisted and Totally Laparoscopic Distal Gastrectomy: The Short-Term Outcome at a Low Volume Center
- Laparoscopy-assisted Total Gastrectomy with Pancreas-preserving Splenectomy for Early Gastric Cancer: A Case Report
- Non-Randomized Confirmatory Trial of Laparoscopy-Assisted Total Gastrectomy and Proximal Gastrectomy with Nodal Dissection for Clinical Stage I Gastric Cancer: Japan Clinical Oncology Group Study JCOG1401
- Morbidity of Laparoscopic Assisted Gastrectomy for Early Gastric Cancer
