Image-based Approach for Surgical Resection of Gastric Submucosal Tumors
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. wjhyung@yuhs.ac
- 2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 4Brain Korea 21 Project for Medical Science, Yonsei University College of Medicine, Seoul, Korea.
Abstract
- PURPOSE
This study was done to evaluate the usefulness of preoperative computed tomography (CT) and intraoperative laparoscopic ultrasound to facilitate treatment of gastric submucosal tumors.
MATERIALS AND METHODS
The feasibility of laparoscopic wedge resection as determined by CT findings of tumor size, location, and growth pattern was correlated with surgical findings in 89 consecutive operations. The role of laparoscopic ultrasound for tumor localization was analyzed.
RESULTS
Twenty-three patients were considered unsuitable for laparoscopic wedge resection because of large tumor size (N=13) or involvement of the gastroesophageal junction (N=9) or pyloric channel (N=1). Laparoscopic wedge resection was not attempted in 11 of these patients because of large tumor size. Laparoscopic wedge resection was successfully performed in 65 of 66 (98.5%) patients considered suitable for this procedure. Incorrect interpretation of preoperative CT resulted in a change of surgery type in seven patients (7.9%): incorrect CT diagnosis on gastroesophageal junction involvement (N=6) and on growth pattern (N=1). In 18 patients without an exophytic growth pattern, laparoscopic ultrasound was necessary and successfully localized all lesions.
CONCLUSIONS
Preoperative CT and laparoscopic ultrasound are useful for surgical planning and tumor localization in laparoscopic wedge resection.
Keyword
MeSH Terms
Figure
-

Fig. 1 Image-based approach for laparoscopic wedge resection. SMT = submucosal tumor; LUS = laparoscopic ultrasound.
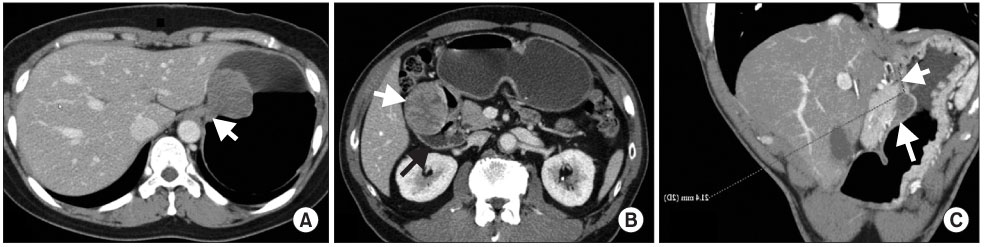
Fig. 2 Estimation of the involvement of the gastric extremities. (A) A 49-year-old woman with pathologically confirmed true leiomyoma. Gastroesophageal junction involvement was found (arrow). Thus, this patient underwent laparoscopic total gastrectomy. (B) A 69-year-old man with pathologically confirmed gastrointestinal stromal tumor. This patient underwent laparoscopic subtotal gastrectomy due to pyloric channel involvement of the tumor (white and black arrows). (C) A 46-year-old woman with pathologically confirmed gastrointestinal stromal tumor (long arrow) in the gastric upper body. The distance between the gastroesophageal junction and the proximal tumor margin was measured as 2.1 cm (short arrow). This patient was regarded as acceptable for laparoscopic wedge resection and underwent the surgery.
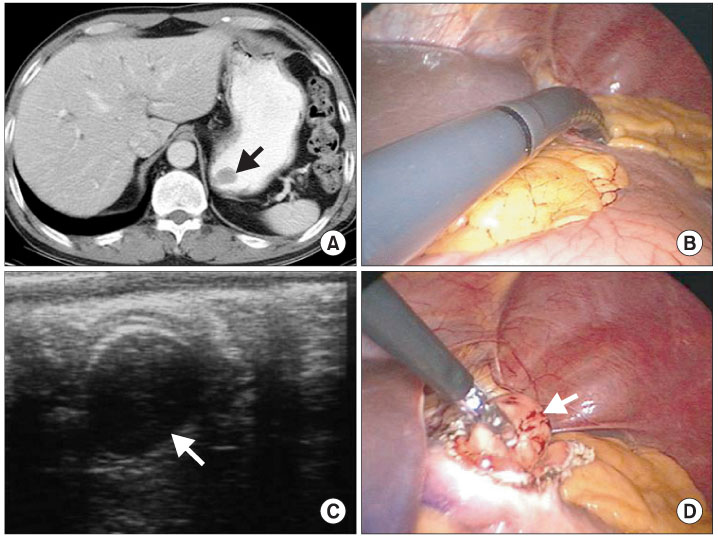
Fig. 3 Use of laparoscopic ultrasound for laparoscopic localization. (A) CT imaging demonstrated a 1.5-cm intraluminal lesion without exophytic component in gastric fundus (arrow). (B) The lesion was not detected by laparoscope. LUS probe were searching for the lesion. (C) It was easily detected by laparoscopic ultrasound (arrow). (D) Gastrotomy was performed with a dissector at the site localized by laparoscopic ultrasound. The gastrotomy site accurately coincided with the lesion (arrow). The lesion was easily resected. CT = computer tomography; LUS = laparoscopic ultrasound.

Fig. 4 Intraoperative results of 23 patients deemed not suitable for laparoscopic wedge resection based on preoperative CT findings. CT = computed tomography.
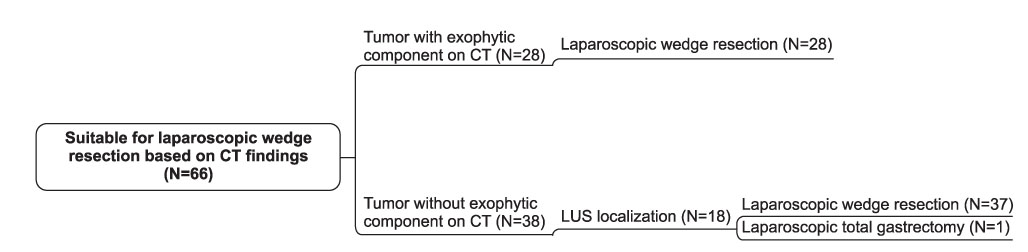
Fig. 5 Intraoperative results of 66 patients deemed suitable for laparoscopic wedge resection based on preoperative CT findings. CT = computed tomography; LUS = laparoscopic ultrasound.
Reference
-
1. Polkowski M. Endoscopic ultrasound and endoscopic ultrasound-guided fine-needle biopsy for the diagnosis of malignant submucosal tumors. Endoscopy. 2005. 37:635–645.
Article2. Kang JH, Lim JS, Kim JH, Hyung WJ, Chung YE, Choi JY, et al. Role of EUS and MDCT in the diagnosis of gastric submucosal tumors according to the revised pathologic concept of gastrointestinal stromal tumors. Eur Radiol. 2009. 19:924–934.
Article3. Choi YB, Oh ST. Laparoscopy in the management of gastric submucosal tumors. Surg Endosc. 2000. 14:741–745.
Article4. Matthews BD, Walsh RM, Kercher KW, Sing RF, Pratt BL, Answini GA, et al. Laparoscopic vs open resection of gastric stromal tumors. Surg Endosc. 2002. 16:803–807.
Article5. Avital S, Brasesco O, Szomstein S, Liberman M, Rosenthal R. Technical considerations in laparoscopic resection of gastric neoplasms. Surg Endosc. 2003. 17:763–765.
Article6. Hepworth CC, Menzies D, Motson RW. Minimally invasive surgery for posterior gastric stromal tumors. Surg Endosc. 2000. 14:349–353.
Article7. Hiki N, Yamamoto Y, Fukunaga T, Yamaguchi T, Nunobe S, Tokunaga M, et al. Laparoscopic and endoscopic cooperative surgery for gastrointestinal stromal tumor dissection. Surg Endosc. 2008. 22:1729–1735.
Article8. Hyung WJ, Lim JS, Cheong JH, Kim J, Choi SH, Noh SH. Laparoscopic resection of a huge intraluminal gastric submucosal tumor located in the anterior wall: eversion method. J Surg Oncol. 2005. 89:95–98.
Article9. Ibrahim IM, Silvestri F, Zingler B. Laparoscopic resection of posterior gastric leiomyoma. Surg Endosc. 1997. 11:277–279.
Article10. Otani Y, Ohgami M, Igarashi N, Kimata M, Kubota T, Kumai K, et al. Laparoscopic wedge resection of gastric submucosal tumors. Surg Laparosc Endosc Percutan Tech. 2000. 10:19–23.
Article11. Hyung WJ, Lim JS, Cheong JH, Lee YC, Noh SH. Tumor localization using laparoscopic ultrasound for a small submucosal tumor. J Surg Oncol. 2004. 86:164–166.
Article12. Ohgami M, Otani Y, Kumai K, Kubota T, Kim YI, Kitajima M. Curative laparoscopic surgery for early gastric cancer: five years experience. World J Surg. 1999. 23:187–192.
Article13. Hyung WJ, Lim JS, Cheong JH, Kim J, Choi SH, Song SY, et al. Intraoperative tumor localization using laparoscopic ultrasonography in laparoscopic-assisted gastrectomy. Surg Endosc. 2005. 19:1353–1357.
Article14. Ba-Ssalamah A, Prokop M, Uffmann M, Pokieser P, Teleky B, Lechner G. Dedicated multidetector CT of the stomach: spectrum of diseases. Radiographics. 2003. 23:625–644.
Article15. Horton KM, Fishman EK. Current role of CT in imaging of the stomach. Radiographics. 2003. 23:75–87.
Article16. Santambrogio R, Montorsi M, Schubert L, Pisani Ceretti A, Costa M, Moroni E, et al. Laparoscopic ultrasound-guided resection of gastric submucosal tumors. Surg Endosc. 2006. 20:1305–1307.
Article17. Aogi K, Hirai T, Mukaida H, Toge T, Haruma K, Kajiyama G. Laparoscopic resection of submucosal gastric tumors. Surg Today. 1999. 29:102–106.
Article18. Demetri GD, Benjamin RS, Blanke CD, Blay JY, Casali P, Choi H, et al. NCCN Task Force. NCCN Task Force report: management of patients with gastrointestinal stromal tumor (GIST)--update of the NCCN clinical practice guidelines. J Natl Compr Canc Netw. 2007. 5:Suppl 2. S1–S29.
Article19. Hyung WJ, Song C, Cheong JH, Choi SH, Noh SH. Percutaneous needle decompression during laparoscopic gastric surgery: a simple alternative to nasogastric decompression. Yonsei Med J. 2005. 46:648–651.
Article20. Lee MW, Kim SH, Kim YJ, Lee JM, Lee JY, Park EA, et al. Gastrointestinal stromal tumor of the stomach: preliminary results of preoperative evaluation with CT gastrography. Abdom Imaging. 2008. 33:255–261.
Article21. Beretvas RI, Ponsky J. Endoscopic marking: an adjunct to laparoscopic gastrointestinal surgery. Surg Endosc. 2001. 15:1202–1203.
Article22. Park DJ, Lee HJ, Kim SG, Jung HC, Song IS, Lee KU, et al. Intraoperative gastroscopy for gastric surgery. Surg Endosc. 2005. 19:1358–1361.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Factors Associated with Operation Time of Laparoscopic Wedge Resection for Gastric Submucosal Tumors
- The Single Incision Laparoscopic Intragastric Wedge Resection of Gastric Submucosal Tumor
- Gastric Glomus Tumor
- Endoscopic and Laparoscopic Full-Thickness Resection of Endophytic Gastric Submucosal Tumors Very Close to the Esophagogastric Junction
- Wedge Resection of the Stomach for Gastric Submucosal Tumors: Laparoscopic vs. Open
