Electrolyte Blood Press.
2016 Dec;14(2):35-37. 10.5049/EBP.2016.14.2.35.
A Case of Isolated Glycosuria Mediated by an SLC5A2 Gene Mutation and Characterized by Postprandial Heavy Glycosuria Without Salt Wasting
- Affiliations
-
- 1Department of Internal Medicine, Eulji University Hospital, Eulji University College of Medicine, Daejeon, Korea.
- 2Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. kwon@chungbuk.ac.kr
- KMID: 2369610
- DOI: http://doi.org/10.5049/EBP.2016.14.2.35
Abstract
- Familial renal glycosuria (FRG) is an inherited disorder characterized by persistent glycosuria in the absence of hyperglycemia. It is caused by mutations in the sodium-glucose co-transporter, leading to increase in the renal excretion of glucose and sodium. However, there have been no studies on the role of fasting and postprandial changes in the urinary sodium excretion in patients with FRG. We report a case of renal glycosuria, which was confirmed by a SLC5A2 mutation via gene sequencing, and compared the postprandial urinary glucose and sodium excretion. A 26-year-old man sometimes experienced glycosuria on routine screening; however, other laboratory findings were normal. His fasting and postprandial urinary glucose excretion levels were 295mg/dL and 2,170mg/dL, respectively. The fasting and postprandial urinary sodium excretion levels were 200mEq/L and 89mEq/L, respectively. In patients with FRG, excessive diuresis might be prevented by a compensatory mechanism that reduces postprandial sodium excretion.
MeSH Terms
Figure
-
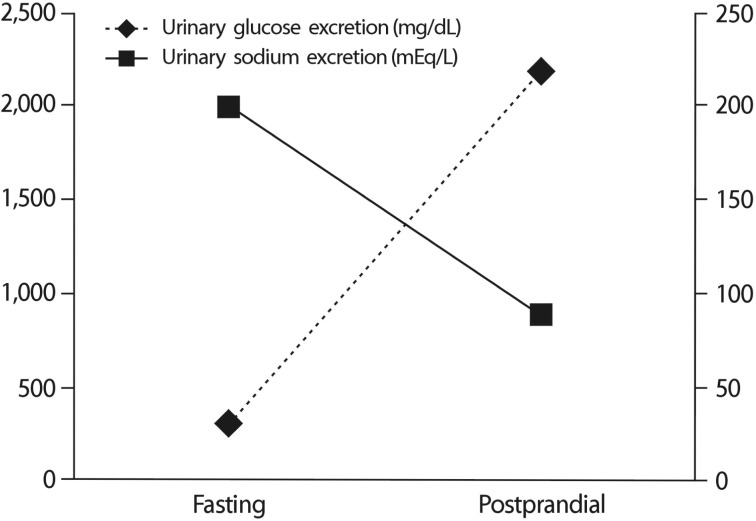
Fig. 1 Changes in the fasting and postprandial urinary sodium and glucose excretion in a patient with familial renal glycosuria.
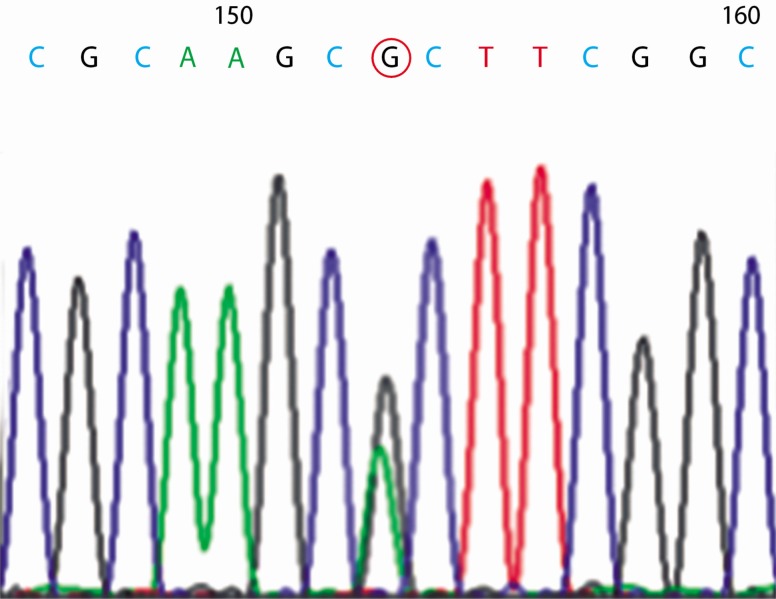
Fig. 2 Sequence analysis of exon 4 of the SGLT2 gene from the study patient. Circles indicate the c.395 position, showing a heterozygous alteration of G>A.
Reference
-
1. Kawasoe M, Kawasoe S, Maruguchi Y. The mechanism of blood pressure-lowering effect of sodium-glucose cotransporter 2 inhibitors in patients with obese type 2 diabetes mellitus. J Am Coll Cardiol. 2016; 67(13_S):1940.
Article2. Baker WL, Smyth LR, Riche DM, Bourret EM, Chamberlin KW, White WB. Effects of sodium-glucose co-transporter 2 inhibitors on blood pressure: a systematic review and meta-analysis. J Am Soc Hypertens. 2014; 8:262–275. PMID: 24602971.
Article3. Wells RG, Mohandas TK, Hediger MA. Localization of the Na/glucose cotransporter gene SGLT2 to human chromosome 16 close to the centromere. Genomics. 1993; 17:787–789. PMID: 8244402.
Article4. Santer R, Kinner M, Schneppenheim R, Hillebrand G, Kemper M, Ehrich J. The molecular basis of renal glucosuria: mutations in the gene for a renal glucose transporter (SGLT2). J Inherit Metab Dis. 2000; 23(Supp 1):178.5. Santer R, Kinner M, Lassen CL, Schneppenheim R, Eggert P, Bald M, Brodehl J, Daschner M, Ehrich JH, Kemper M, Li Volti S, Neuhaus T, Skovby F, Swift PG, Schaub J, Klaerke D. Molecular analysis of the SGLT2 gene in patients with renal glycosuria. J Am Soc Nephrol. 2003; 14:2873–2882. PMID: 14569097.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Novel SLC5A2 Mutations and Genetic Characterization in Korean Patients with Familial Renal Glucosuria
- Prevalence of Diabetes Mellitus and Glycosuria in School Children
- A case of Fanconi syndrome
- Diagnostic Significance of the Urine-Stick Test in Middle and High School Children in Seoul
- A Case of the Fanconi Syndrome with Nephrocalcinosis
